Downloaded 817 times
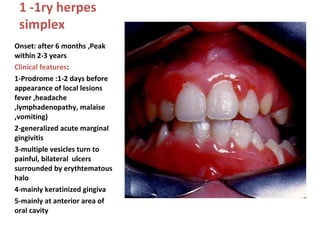

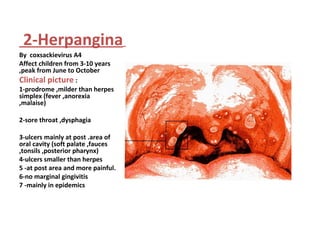

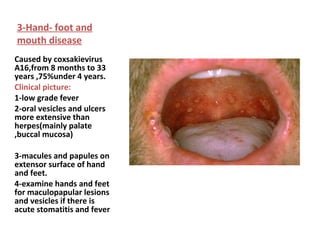

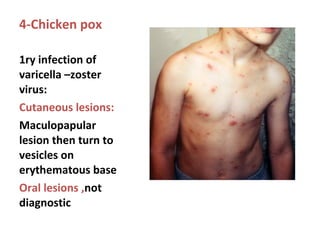



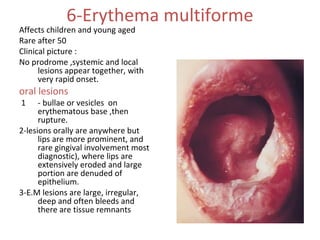

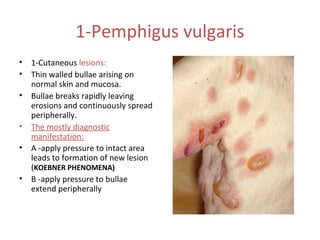
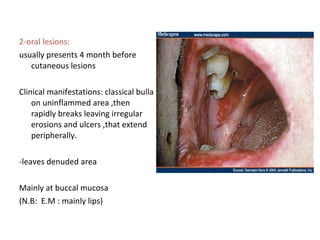
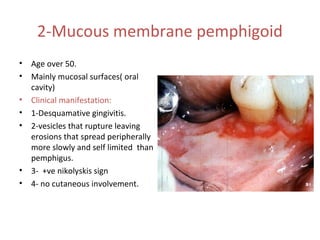

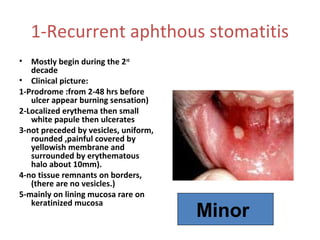



1. Acute multiple oral ulcers can be caused by primary herpes simplex infection, herpangina caused by coxsackievirus A4, hand-foot-and-mouth disease caused by coxsackievirus A16, chickenpox caused by varicella zoster virus, or herpes zoster infection. 2. Chronic multiple ulcers can be caused by pemphigus vulgaris, characterized by thin-walled bullae and erosions that extend peripherally, or mucous membrane pemphigoid, presenting mainly with desquamative gingivitis and erosions. 3. Recurrent oral ulcers include recurrent aphthous stomat






































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







