Downloaded 201 times


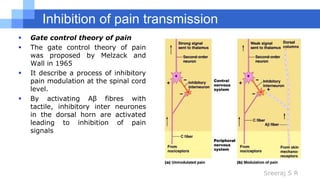
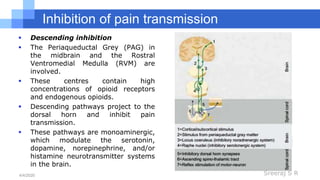
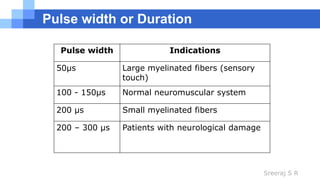


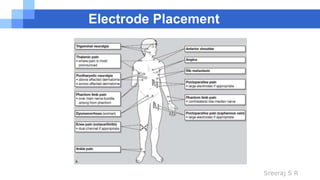
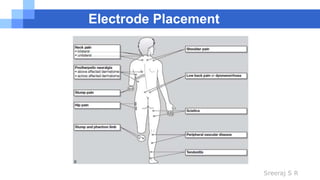
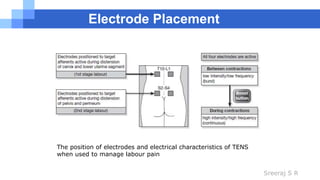

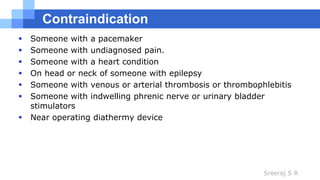


Transcutaneous Electrical Nerve Stimulation (TENS) is a method of electrical stimulation that aims to provide pain relief by exciting sensory nerves and stimulating the pain gate mechanism and/or opioid system. TENS works through several mechanisms including activation of pain-gating mechanisms in the spinal cord and stimulation of the descending pain suppression system and endogenous opioid release. Different TENS waveforms, frequencies, pulse widths and intensities can be used depending on the type of pain and desired effects. Common types of TENS include conventional high frequency TENS and acupuncture-like low frequency TENS. Care must be taken with electrode placement and TENS is generally contraindicated for those with pacemakers or heart conditions.























































































