Download to read offline
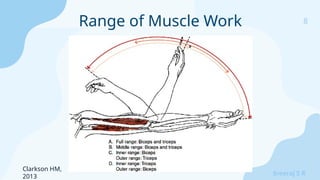

![21
Sreeraj S R
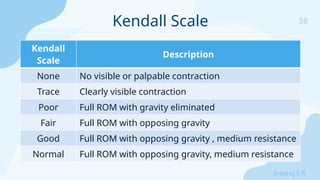
● Garner JC, Blackburn T, Weimar W, Campbell B. Comparison of
electromyographic activity during eccentrically versus concentrically
loaded isometric contractions. Journal of Electromyography and
Kinesiology [Internet]. 2008 Jun;18(3):466–71. Available from:
https://exss.unc.edu/wp-content/uploads/sites/779/2013/01/garner_
2008_jek.pdf
For concentrically loaded isometric muscle contraction vs
eccentrically loaded isometric muscle contraction](https://image.slidesharecdn.com/manualmuscletestingsrs-241026082220-5368f1cb/85/Manual-Muscle-Testing_Understanding-the-Basics_SRS-pptx-21-320.jpg)
![40
Sreeraj S R
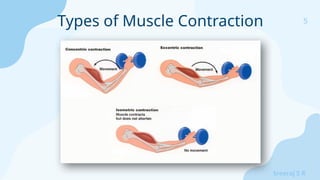
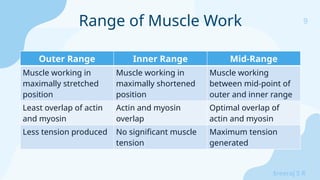
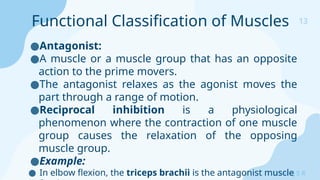
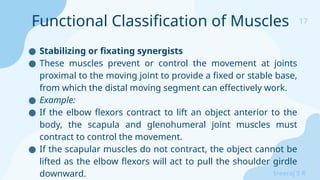
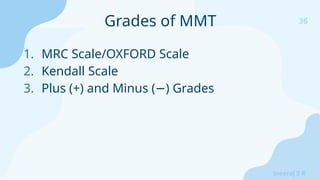
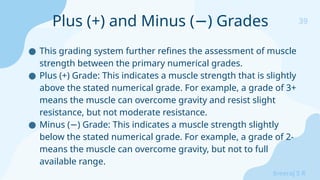
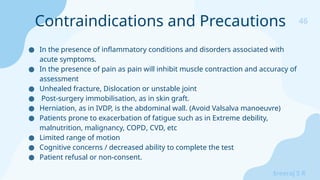
Comparison of MMT grades
Medical
Research
Council[4]
Daniels and
Worthingham[5]
Kendall and
McCreary[6]
Explanation
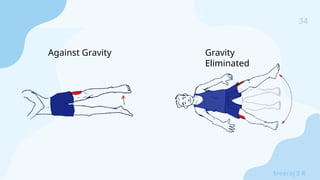
5 Normal(N) 100% Holds test position against
maximal resistance
4+ Good + (G+) Holds test position against moderate
to strong pressure
4 Good(G) 80% Holds test position against
moderate resistance
4- Good – (G-) Holds test position against slight to
moderate pressure
3+ Fair + (F+) Holds test position against slight
resistance
3 Fair (F) 50% Holds test position against
gravity
3- Fair- (F-) Gradual release from test position
2+ Poor + (P+) Moves through partial ROM against
gravity OR Moves through complete
ROM gravity eliminated and holds
against pressure
2 Poor(P) 20% Able to move through full ROM
gravity eliminated
2- Poor – (P-) Moves through partial ROM gravity
eliminated
1 Trace(T) 5% No visible movement; palpable
or observable tendon
prominence/flicker contraction
0 0 0% No palpable or observable
muscle contraction](https://image.slidesharecdn.com/manualmuscletestingsrs-241026082220-5368f1cb/85/Manual-Muscle-Testing_Understanding-the-Basics_SRS-pptx-40-320.jpg)


![48
Sreeraj S R
1. Houglum PA. Chapter 7. Muscle Strength and Endurance. Therapeutic Exercise for
Musculoskeletal Injuries. 3rd Edition. 2010: pp 199-251
2. Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Chapter 1. Fundamental
Concepts. Muscles Testing and Function with Posture and Pain. 5th Edition. Elsevier. 2005: pp 3-47
3. Hislop HJ, Avers D, Brown M. Chapter 1. Principles of Manual Muscle Testing. Daniels and
Worthingham’s Muscle Testing-techniques of Manual Examination and Performance Testing. 9th
Edition. 2014: pp 2-6
4. Hislop HJ, Avers D, Brown M. Chapter 2. Relevance and Limitations of Manual Muscle Testing.
Daniels and Worthingham’s Muscle Testing-techniques of Manual Examination and Performance
Testing. 9th Edition. 2014: pp 12-16
5. Clarkson HM. Principles and Methods. In: Musculoskeletal Assessment: Joint Motion and Muscle
Testing. Philadelphia: Lippincott Williams & Wilkins; 2013. p. 1–54.
6. Naqvi U, Sherman AL. Muscle Strength Grading [Internet]. Nih.gov. StatPearls Publishing; 2023
[cited 2024 Oct 8]. Available from: https://tinyurl.com/y453uwxp
References](https://image.slidesharecdn.com/manualmuscletestingsrs-241026082220-5368f1cb/85/Manual-Muscle-Testing_Understanding-the-Basics_SRS-pptx-48-320.jpg)

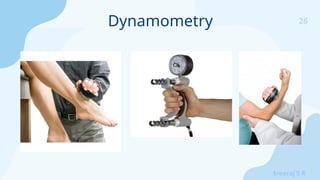
The document discusses manual muscle testing, including definitions of muscle strength, types of contractions (isometric and isotonic), and factors affecting strength. It details various assessment methods such as dynamometry, isokinetic testing, and electromyography, as well as the muscle strength grading systems used to evaluate performance. Additionally, it highlights the importance of controlled testing environments and acknowledges limitations and contraindications associated with muscle strength assessments.
















![J._CONTRAST_BATH_THERAPY[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/j-230713132551-5c45004c-thumbnail.jpg?width=640&height=640&fit=bounds)





































































