
Downloaded 65 times

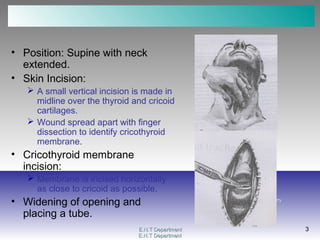


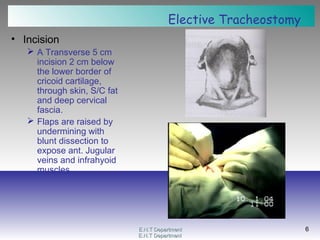



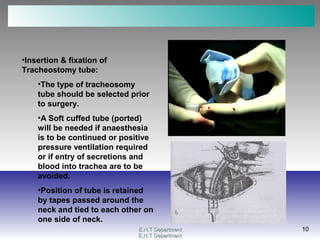


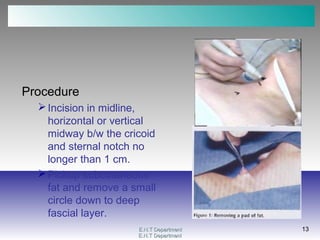
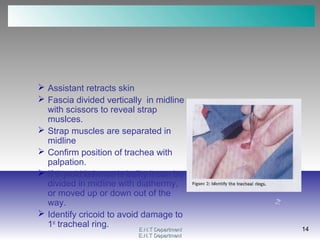
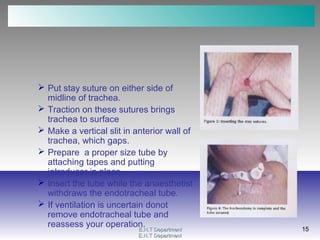

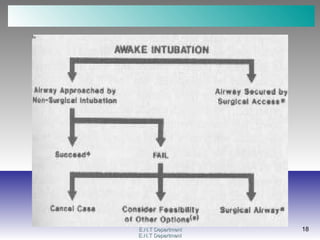

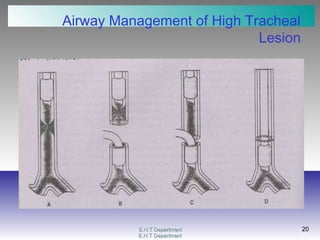





This document provides information on various ENT surgical procedures including laryngotomy, tracheostomy, and tracheal stenosis management. It describes the steps for performing an emergency laryngotomy to open the airway through the cricothyroid membrane. For tracheostomy, it outlines the elective procedure including patient positioning, incision placement below the cricoid cartilage, separating the infrahyoid muscles, and inserting and securing a tracheostomy tube. It also discusses special considerations for pediatric tracheostomy. Tracheal stenosis management techniques include distal tracheal intubation, jet ventilation, extracorporeal membrane oxygenation, and cardiopulmonary bypass.








































































![Introduction to hearing implairment & cochlear implantation]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontohearingimplairmentcochlearimplantation-161111054000-thumbnail.jpg?width=640&height=640&fit=bounds)


































