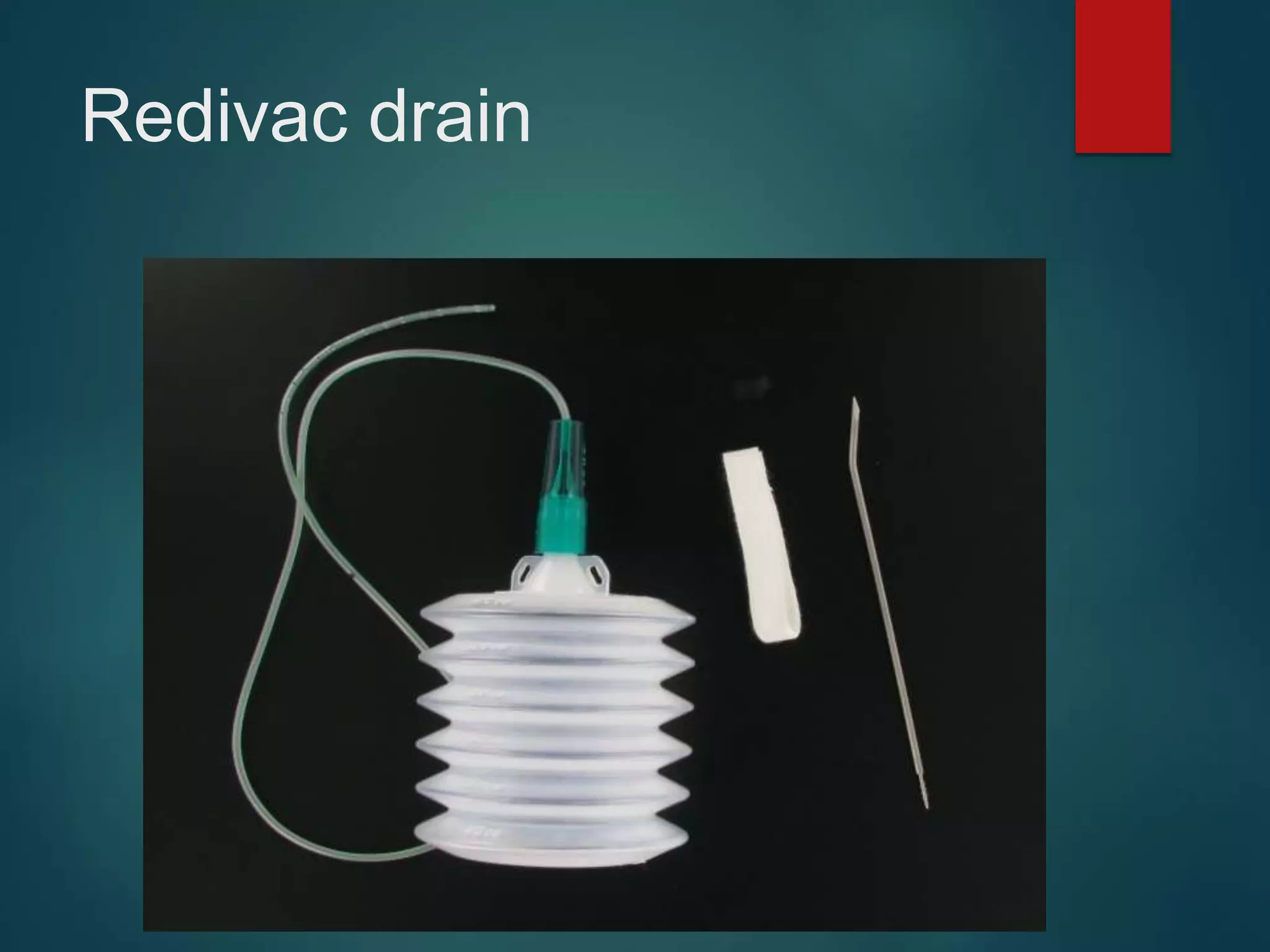
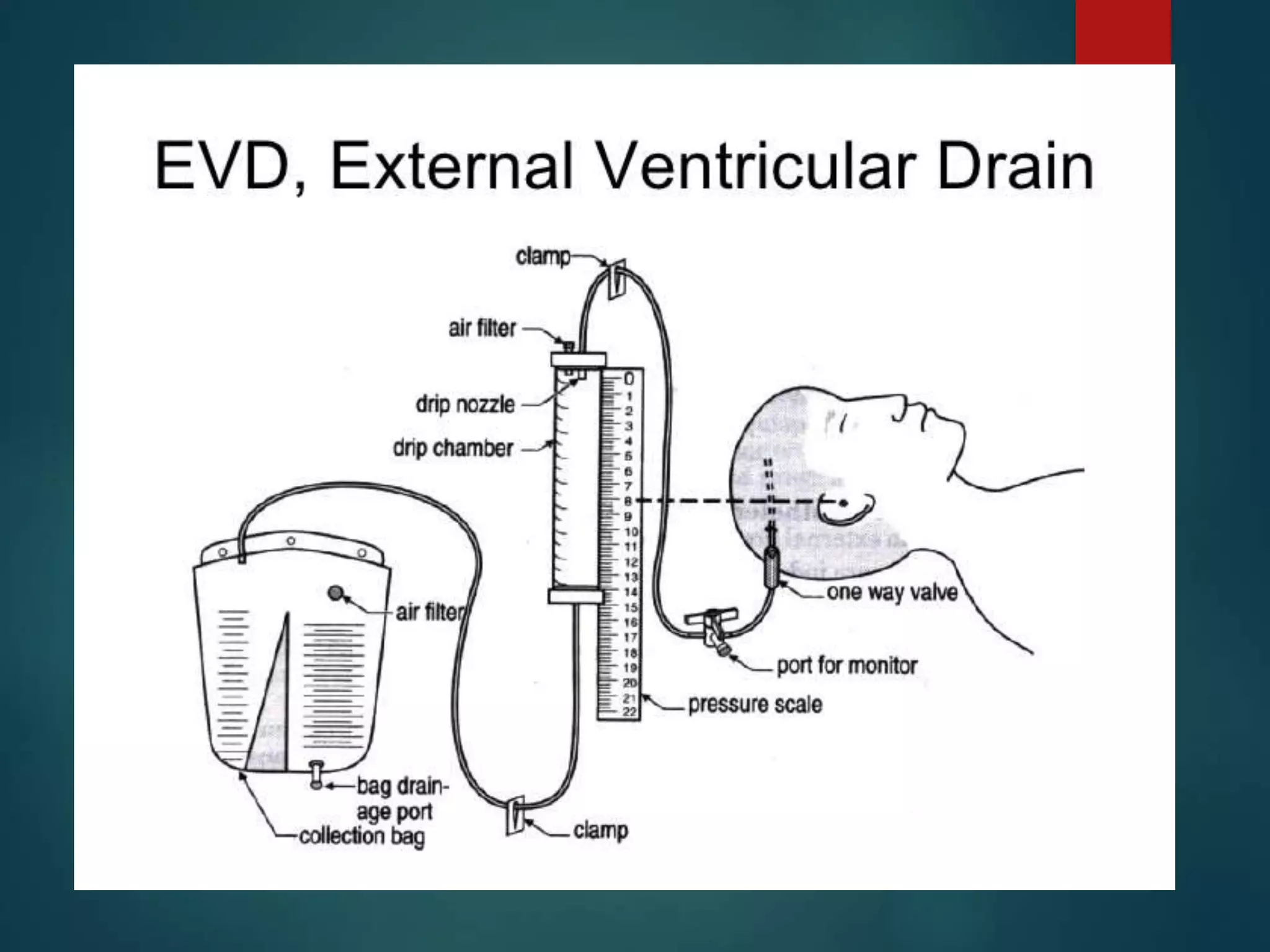
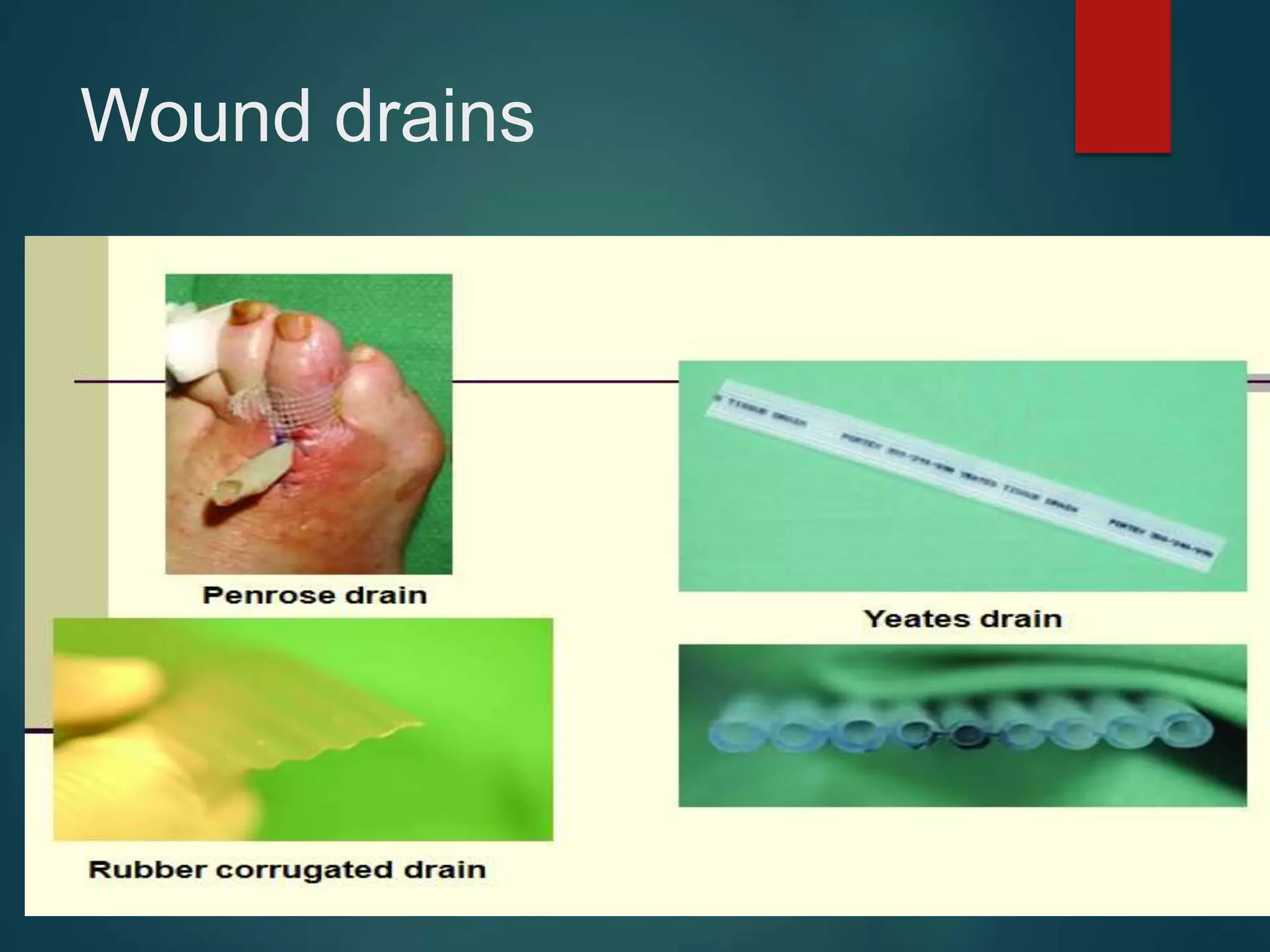
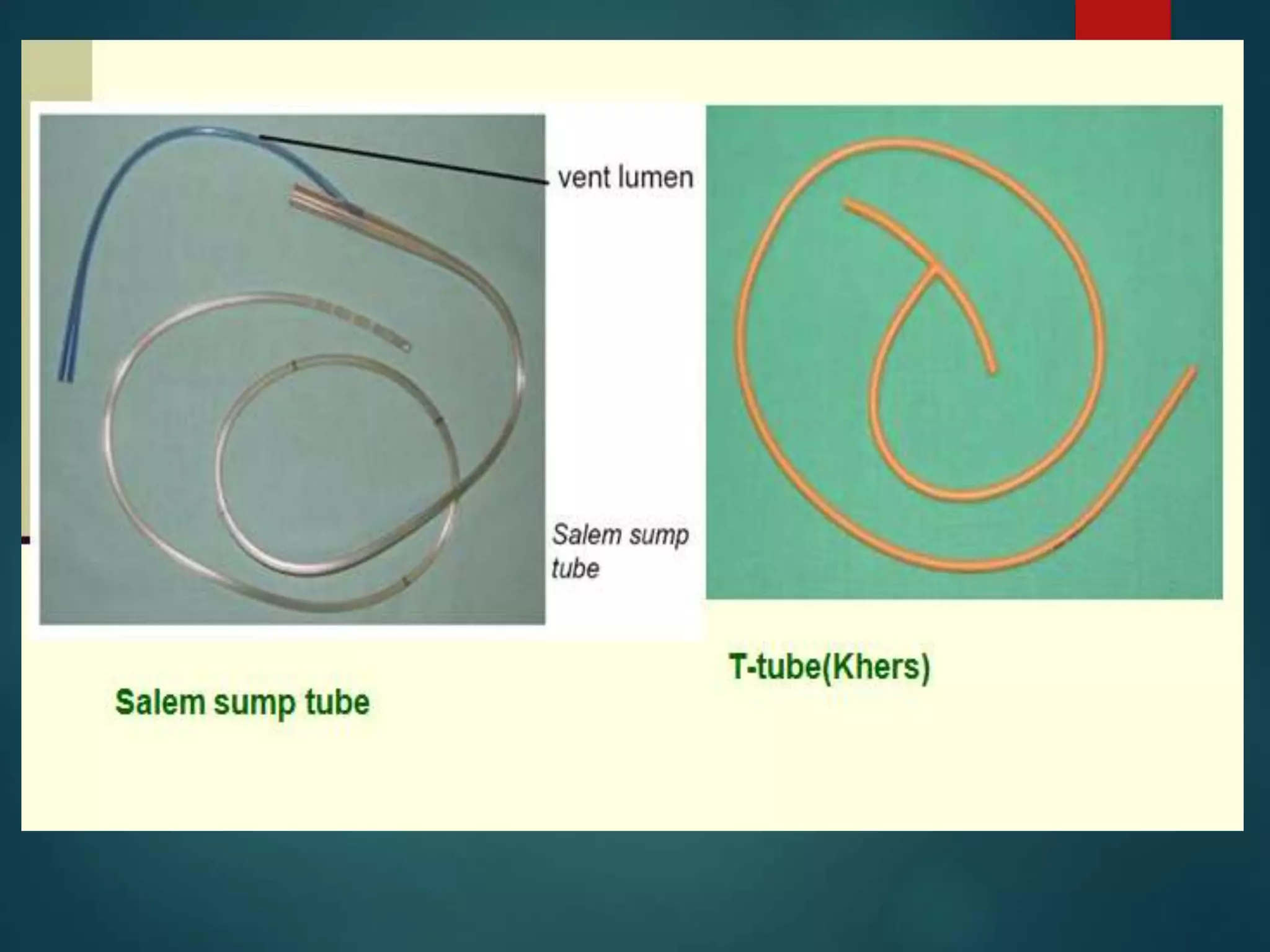
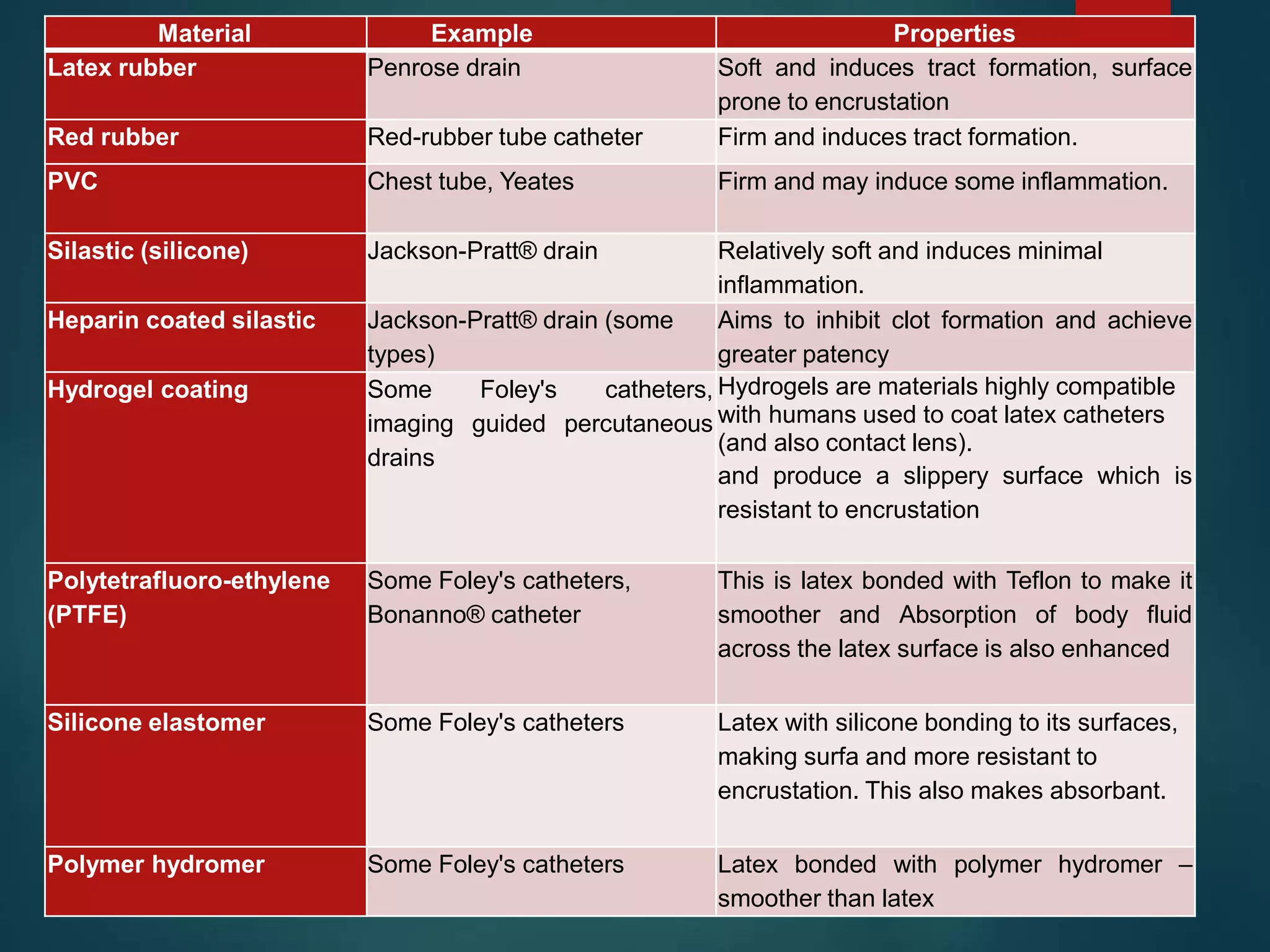
This document provides an overview of surgical drainage systems, including their classification, materials, qualities, use, indications, complications and more. It discusses the types of drainage systems such as active vs passive, open vs closed, and internal vs external. The key types of drain materials are also outlined. The principles of drain use, indications, abuses and complications are summarized. Finally, drain removal techniques are briefly covered.