
Downloaded 993 times




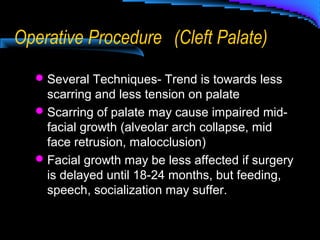
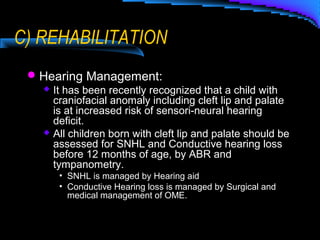

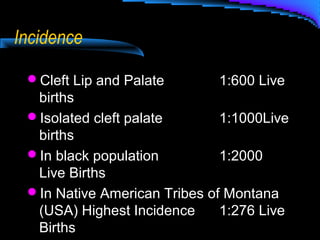
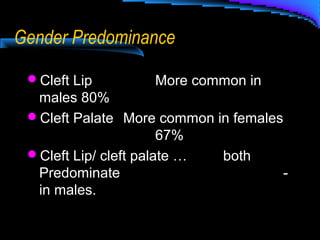
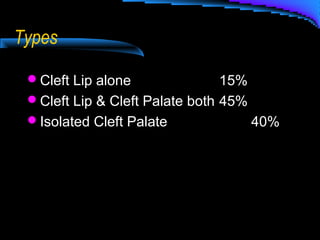
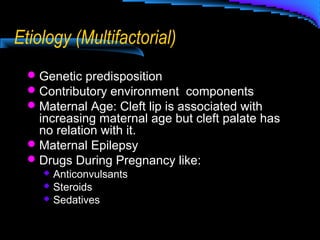




Cleft lip and palate are common birth defects that affect speech, hearing, breathing, and appearance. They require a team-based approach involving multiple specialists like otolaryngologists. The document discusses the management of cleft lip and palate, including the roles of different specialists in examining, diagnosing, and treating issues related to feeding, airway, speech, hearing, and surgery. Surgical techniques aim to restore normal anatomy and function through procedures on the lip and palate.
















































![Introduction to hearing implairment & cochlear implantation]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontohearingimplairmentcochlearimplantation-161111054000-thumbnail.jpg?width=640&height=640&fit=bounds)
























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
