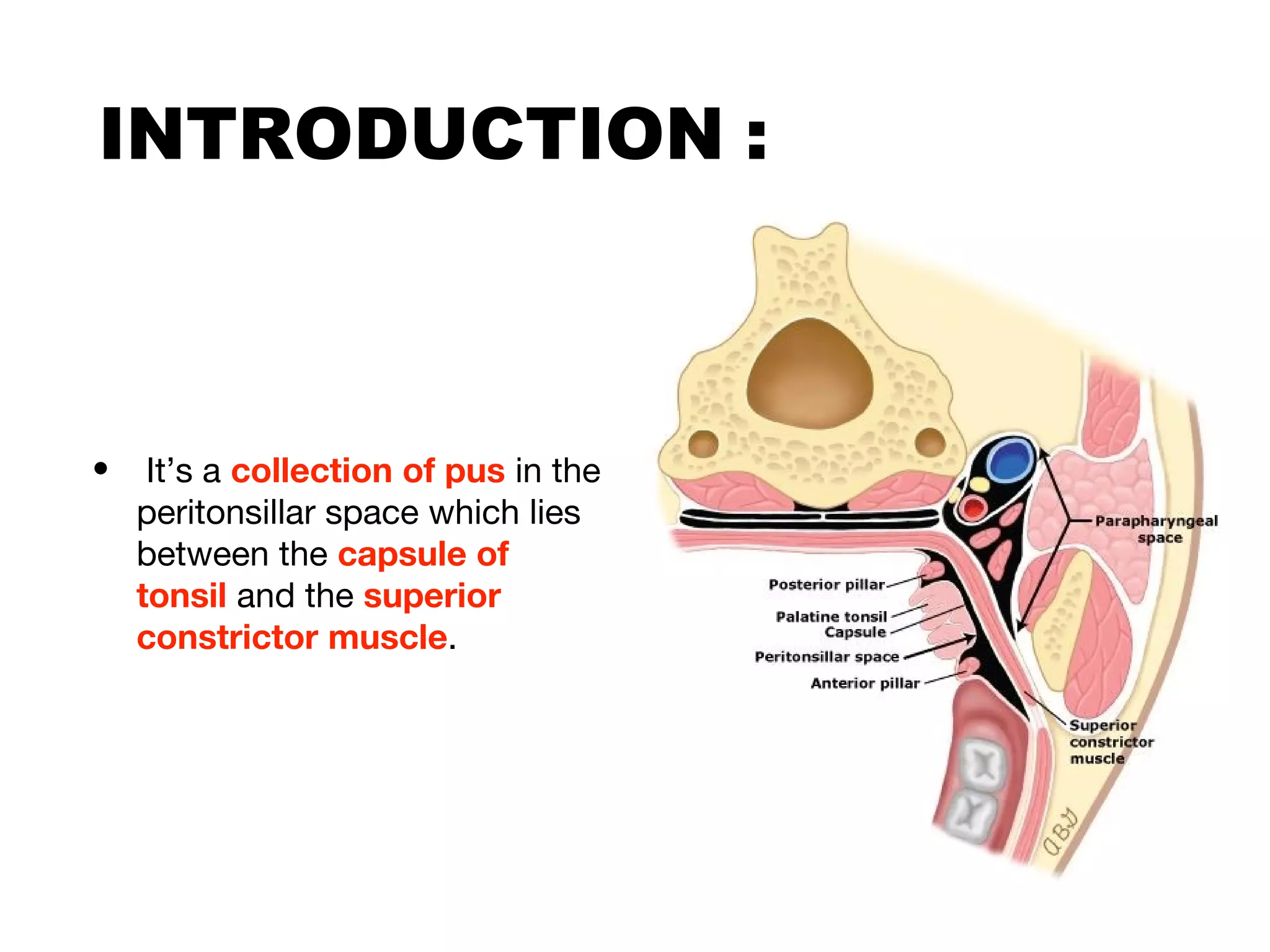
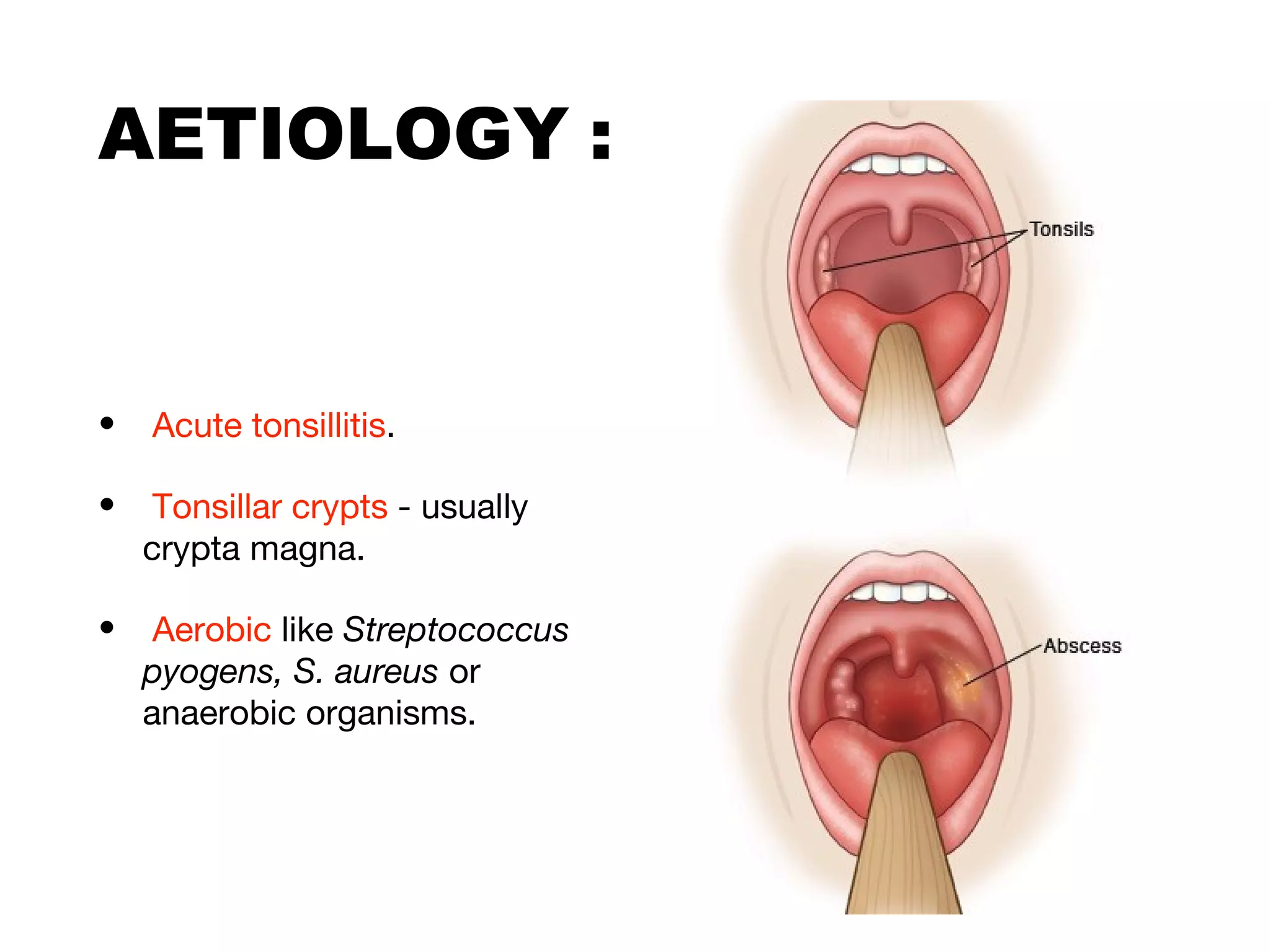
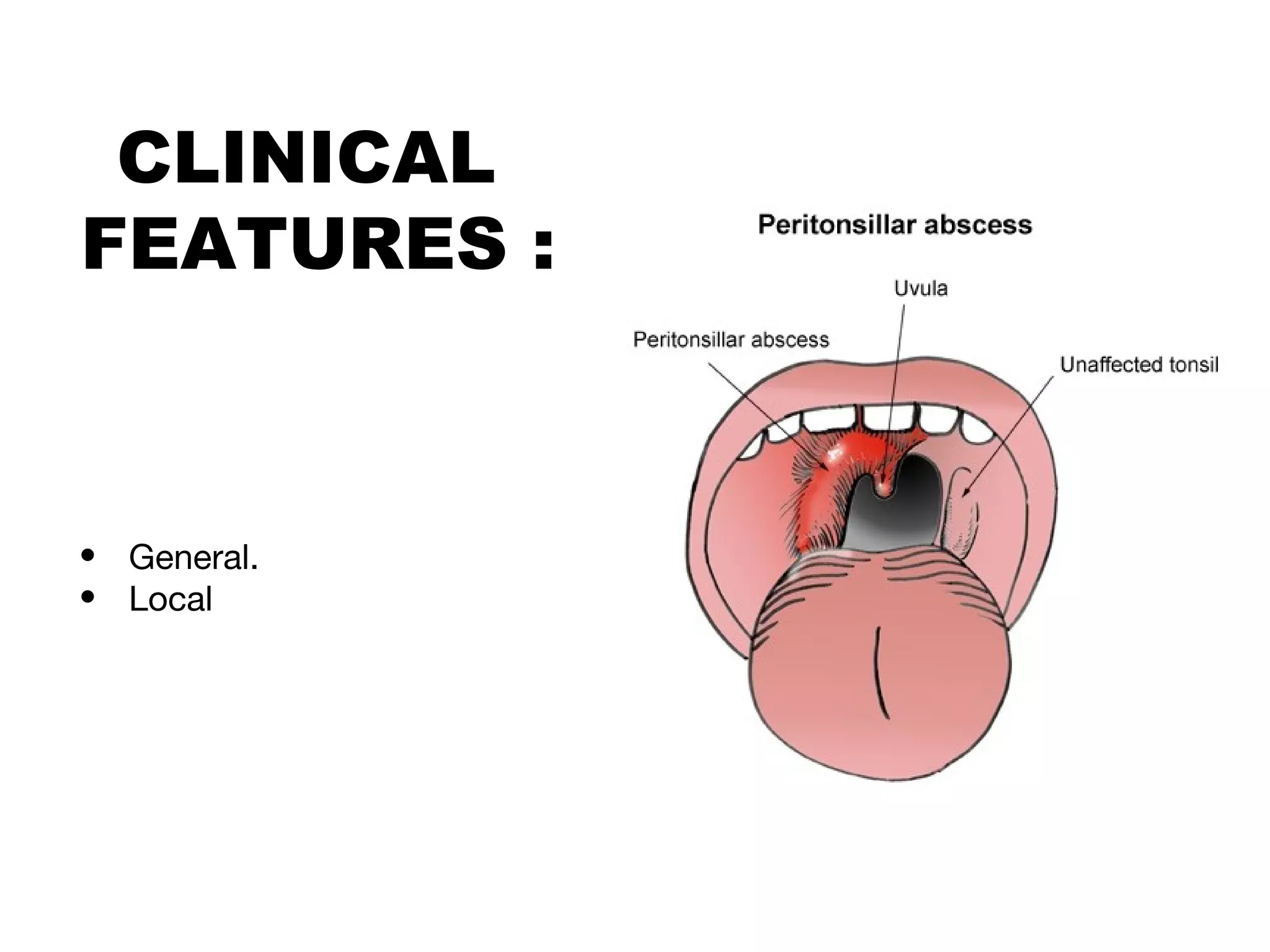
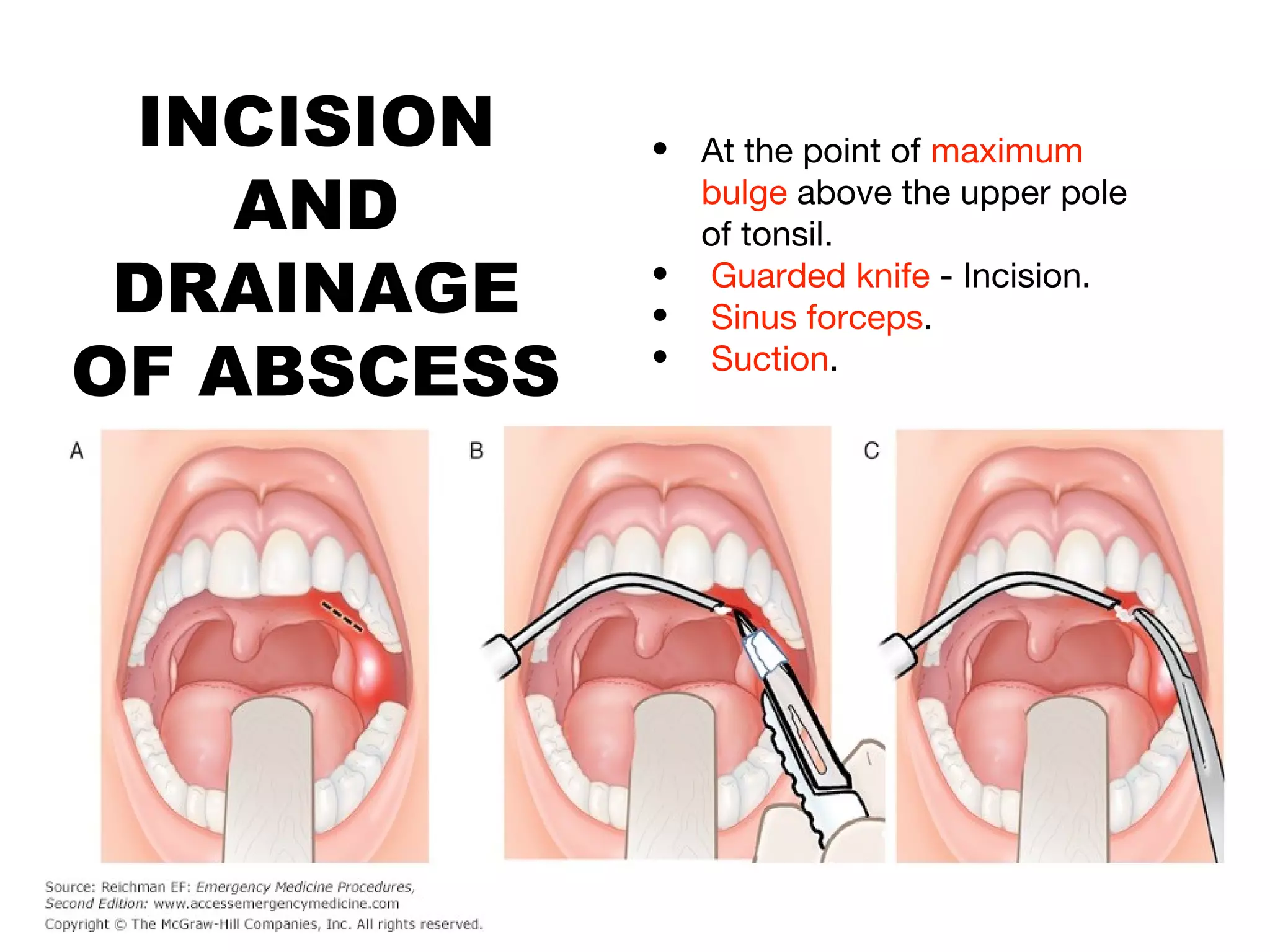
Quinsy, also known as peritonsillar abscess, is a collection of pus in the space between the tonsil capsule and the superior constrictor muscle, usually caused by acute tonsillitis. Symptoms include fever, throat pain, difficulty swallowing, and ear pain on the affected side. On examination, the tonsils and surrounding areas will be swollen and red with mucopus visible. Treatment involves hospitalization, IV fluids, antibiotics, analgesics, and incision and drainage of the abscess.