Downloaded 356 times
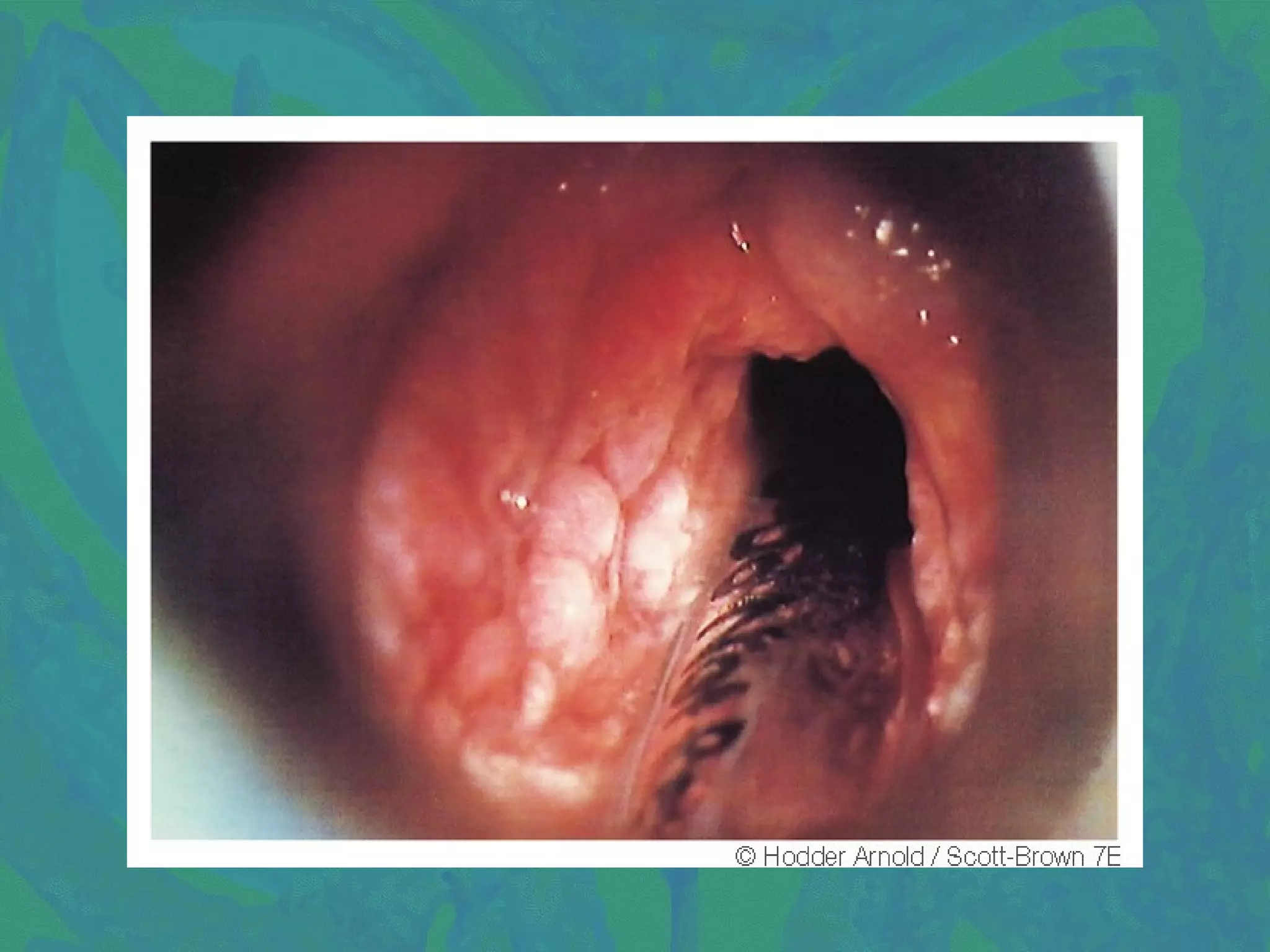

1. Tuberculosis of the larynx commonly affects the posterior larynx, causing submucosal tubercles that can ulcerate, forming undermined ulcers. Symptoms include throat pain, hoarseness, and dysphagia. Diagnosis involves chest X-ray, sputum examination, laryngoscopy, and biopsy. Treatment consists of anti-tubercular drugs, vocal rest, and nutrition supplements. 2. Scleroma of the larynx is caused by Klebsiella rhinoscleromatis and commonly involves the subglottic region, presenting as a smooth red swelling. Diagnosis involves biopsy and culture. Treatment includes antibiotics, steroids, and surgery for stenosis






















































![Inflammatory disorders of larynx [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/inflammatorydisordersoflarynxautosaved-140630024246-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




















































