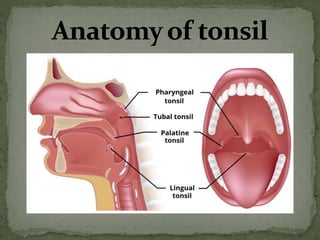
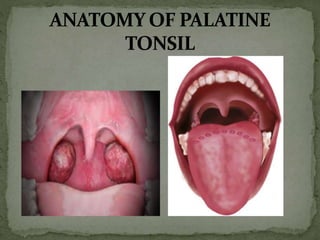
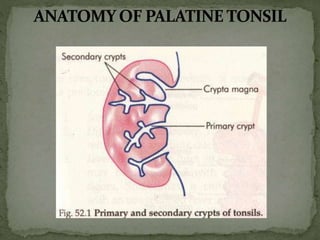
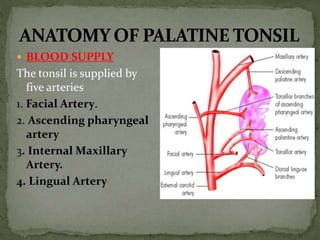
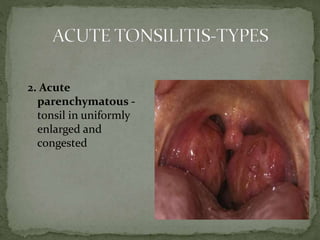
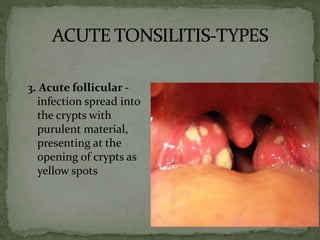
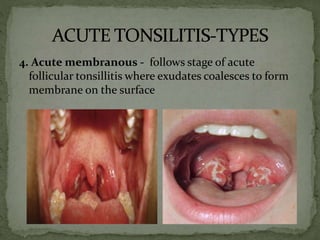
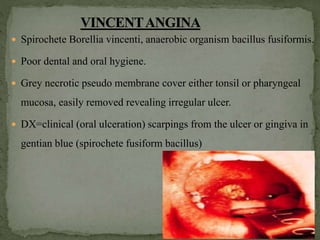
The document discusses the anatomy, blood supply, lymphatic drainage, histology, grading scales, types of tonsillitis, symptoms, signs, investigations, treatment and complications of tonsillitis. It provides details on the tonsils, including that they are paired structures in the oropharynx with crypts on the medial surface. Acute tonsillitis can present as catarrhal, parenchymatous, follicular or membranous depending on the site of infection within the tonsil. Chronic tonsillitis results from recurrent infections and can lead to complications like peritonsillar abscesses if left untreated.

































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




