Downloaded 23 times

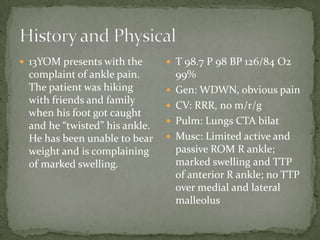

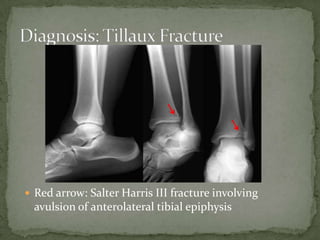
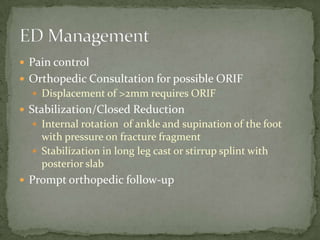
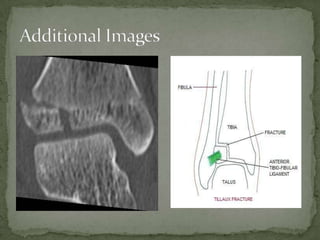
A 13-year-old male presented with ankle pain after twisting his foot while hiking. On examination, he had limited range of motion in his right ankle with marked swelling and tenderness. Radiographs revealed a Salter Harris III fracture involving avulsion of the anterolateral tibial epiphysis. He was treated with pain control, orthopedic consultation for possible open reduction and internal fixation, and stabilization in a long leg cast or splint with orthopedic follow-up.











































































































