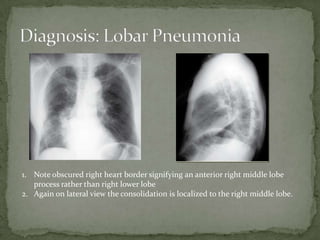
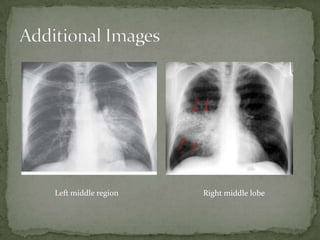
A 76-year-old female presented with worsening dyspnea, cough producing yellow sputum, subjective fevers and chills, weakness and decreased appetite. Her vital signs and physical exam showed signs of infection. Chest x-rays revealed consolidation in the right middle lobe, suggesting lobar pneumonia. She was treated with oxygen, IV fluids, antibiotics and admitted to the hospital based on her condition.











































![Emergency in Urology [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/emergencyuroedmond-140716213857-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































































