Downloaded 349 times

![ Thyroid storm
a life-threatening condition, requiring early recognition and
aggressive therapy in an intensive care unit setting.
During gestation, women with hyperthyroidism should have
their thyroid function checked every 3-4 weeks.
Grave's disease represents the most common cause of
maternal hyperthyroidism during pregnancy
Only 0.2% of gestations are complicated by thyroid storm and
more than 90% of cases are caused by Grave's disease
Increased production of thyroid hormone occurs when
autoantibodies (thyroid-stimulating antibody [TSAb] --
formerly known as LATS [long-acting thyroid stimulator])
against TSH receptors -- acts as TSH agonists.](https://image.slidesharecdn.com/thyroiddiseaseandpregnancyppt-151016132423-lva1-app6891/85/Thyroid-disease-and-pregnancy-ppt-35-320.jpg)

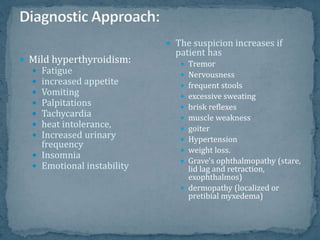
Thyroid disease, specifically hyperthyroidism, is a significant concern during pregnancy, with risks including preterm birth, heart failure, and thyroid storm. The most common cause is Graves' disease, which leads to elevated thyroid hormones due to autoimmune factors. Management involves careful monitoring and treatment, including the use of medications like propylthiouracil and methimazole, while avoiding contraindicated therapies such as radioactive iodine during pregnancy.























































































