Hypothyroidism inpregnancy
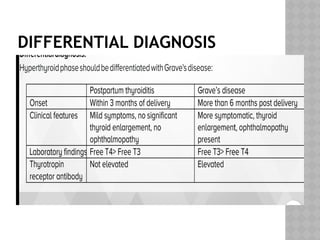
Hyperthyroidism in pregnancy
Postpartum thyroiditis
4.
THYROID ANATOMY AND
PREGNANCY
Thyroid gland undergoes moderate
enlargement during pregnancy caused by
glandular hyperplasia and increased
vascularity
But it will not cause significant thyromegaly
so any goiter in pregnancy should be
investigated .
5.
THYROID PHYSIOLOGY AND
PREGNANCY
To meet the increased metabolic needs
during a normal pregnancy ,there are
changes in thyroid physiology.
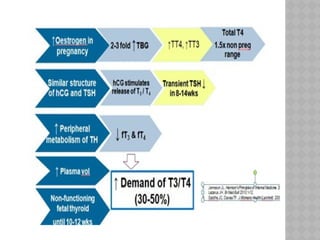
An increase in thyroxine-binding globulin
(TBG) occurs upto 20 weeks and then
stabilizes at approx. double the baseline
value .
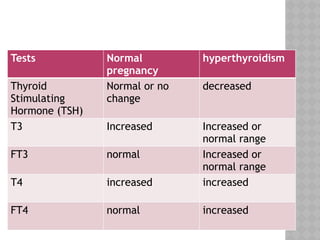
Increase in total T3 and total T4
Decrease in TSH
Normal free T3 ad free T4
6.
THYROID FUNCTION ANDHCG
Alpha subunit of both TSH and hCG are similar
hCG has weak thyroid-stimulating activity
High serum hCG levels cause high thyroid hormone
levels
80% pregnant women –TSH level decreases
7.
Serum hCGconcentrations increase soon
after fertilization and peak at 10 to 12 weeks
During this peak total serum T4 and T3
increases while free T3 and T4 remains
within normal range ,TSH level decreases
Second and third trimester- there is gradual
return of TSH towards normal range
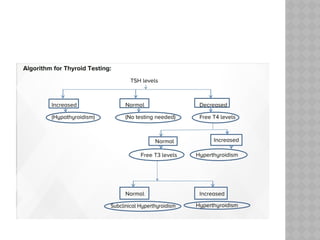
Hence in pregnancy we measure TSH and
free T4 and not total T4
9.
IODINE STATUS INPREGNANCY
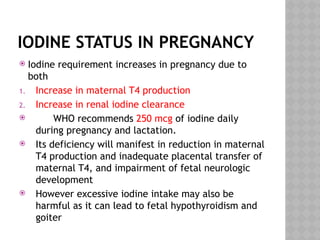
Iodine requirement increases in pregnancy due to
both
1. Increase in maternal T4 production
2. Increase in renal iodine clearance
WHO recommends 250 mcg of iodine daily
during pregnancy and lactation.
Its deficiency will manifest in reduction in maternal
T4 production and inadequate placental transfer of
maternal T4, and impairment of fetal neurologic
development
However excessive iodine intake may also be
harmful as it can lead to fetal hypothyroidism and
goiter
10.
THYROID FUNCTION INTHE FETUS
During the 10 to 12 weeks of gestation, fetal
TSH appears and the fetal thyroid is capable of
concentrating iodine and synthesizing T3,T4
However little synthesis occurs until the 18th
to
20th
week thereafter secretion increases
gradually
So maternal thyroid hormones are critical for
growth and nervous system development in the
first trimester
Iodine deficiency is the most common
preventable cause of impaired neurological
development .
CAUSES
Maternal hypothyroidism inpregnancy is due to
1. Autoimmune thyroiditis
2. post-thyroidectomy, prior radioiodine
ablation
3. Iodine deficiency
Chronic autoimmune (Hashimoto’s) thyroiditis
is the commonest cause in pregnancy.
Thyroid antibodies are present in almost 60%
of reproductive age women.
13.
GUIDELINES COUNTRY TRIMESTERSPECIFIC
RECOMMENDED
TSH REF RANGE
ITS Guidelines
2012
India •1st : 0.1-2.5 mIU/L
•2nd :0.2- 3.0mIU/L
•3rd :0.3- 3.0 mIU/L
ETA Guidelines
2014
European •1st : 2.5 mIU/L
•2nd : 3.0mIU/L
•3rd : 3.0 mIU/L
ATA Guidelines
2017
American Use locally derived
Reference ranges
from a specified
Pregnant population
· If the above is not
available use and
upper TSH reference
limit of 4.0 mIU/L
14.
Overt hypothyroidismis increased in serum
TSH (more than 10 mIU/L) with reduced free
T4 level.
Subclinical hypothyroidism is serum TSH level
in the range of 4-10 mIU/L with normal
thyroxine (T4) level.
The incidence of overt hypothyroidism is 0.2-
2.5 % and that of subclinical hypothyroidism
is 2-7%.
15.
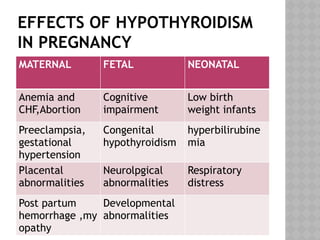
EFFECTS OF HYPOTHYROIDISM
INPREGNANCY
MATERNAL FETAL NEONATAL
Anemia and
CHF,Abortion
Cognitive
impairment
Low birth
weight infants
Preeclampsia,
gestational
hypertension
Congenital
hypothyroidism
hyperbilirubine
mia
Placental
abnormalities
Neurolpgical
abnormalities
Respiratory
distress
Post partum
hemorrhage ,my
opathy
Developmental
abnormalities
16.
Pregnancies inwomen with subclinical
hypothyroidism were 3 times more likely to be
complicated by placental abruption.
Preterm birth was almost 2-fold higher in women
with subclinical hypothyroidism
Lab investigation: TSH,FT3,FT4,anti-TPO
antibodies
Positive anti-thyroid peroxidase (TPO) antibodies
tend to have the highest risk of adverse
pregnancy outcomes
18.
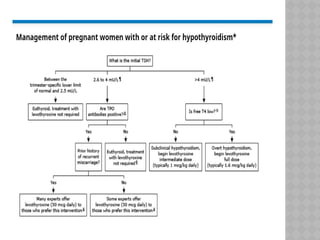
MANAGEMENT OF HYPOTHYROIDISM
Levothyroxine (LT4) dose 1.6-2.0 μg/kg/day.
Maintain the target TSH levels ≤2.5 mIU/L.
In patients with pre-existing hypothyroidism,
Levothyroxine(LT4) dose increased by 30% as
soon as pregnancy is diagnosed.
Regular TSH monitoring (approximately every
4-6 weeks until midgestation and at least
once near 28 weeks gestation) should be
done.
19.
MANAGEMENT OF HYPOTHYROIDISM
POST-PARTUM
Post-delivery the patient should be reverted
back to the pre-pregnant dosage and TSH
levels should be rechecked after 6 weeks.
Patients in whom LT4 is initiated during
pregnancy and the LT4 dose is ≤50 mcg daily
may not require LT4 postpartum.
If LT4 is discontinued, serum TSH should be
evaluated in ~ 6 weeks.
Women with thyroid autoimmunity need
annual monitoring with TSH.
20.
COUNSELLING BEFORE
PREGNANCY
womenwith preexisting hypothyroidism who
are planning to become pregnant should
optimize their thyroid hormone dose
preconception.
the goal preconception serum TSH level is
between the lower reference limit and 2.5
mU/L.
Hyperthyroidism can bedefined as 'Increased
thyroid hormone production due to
overactive thyroid gland'.
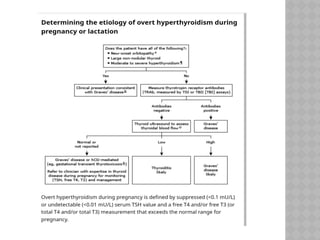
Overt hyperthyroidism : low TSH ,high FT4,FT3
or total T4 &T3 exceeds 1.5times the
nonpregnant range (incidence 0.1-0.4%)
Subclinical hyperthyroidism: low TSH, normal
FT3,FT4 pr total T3 & T4 less than 1.5 times
the nonpregnant range.
transient and normal physiologic finding in
first trimester
Human chorionicgonadotropin (HCG) interacts
and stimulates the TSH receptors in the thyroid
gland thus mimicking an effect of
hyperthyroidism.
During the first trimester of pregnancy, Rising
levels of HCG are noted which result in low or
suppressed TSH values and a mild transient
increase in the levels of T4.
Hence a continuous monitoring is indicated as
the TSH values would further fall back to their
normal range in the second or third trimester
due to decrease in the HCG levels.
25.
CAUSES OF HYPERTHYROIDISMIN PREGNANCY:
Thyrotoxicosis (a clinical condition due to increased
levels of circulating thyroid hormones) in pregnancy may
be due to multiple causes:
Intrinsic disease of the thyroid:
1. Graves' disease
2. Thyroid nodule
3. Sub-acute thyroiditis
Pregnancy Induced (hCG related)
1. Hyperemesis
2. Hydatidiform mole
Miscellaneous:
1. Drug induced
.
26.
Graves' diseaseis one of the most common
causes of a pre-existing hyperthyroidism
which is autoimmune in nature .
It is a syndrome that includes
hyperthyroidism, goiter ,opthalmopathy ,
dermopathy ( pretibial myxedema)
Thyroid stimulating hormone receptor
antibody (TSH RAb) is the reason for the
stimulation of excess thyroid hormone
synthesis and secretion as well as causing
diffuse goiter.
27.
DIAGNOSIS OF HYPERTHYROIDISM
INPREGNANCY
Symptoms:
Sweating, palpitations, heat intolerance,
weight loss or failure to gain weight, nausea
etc.
Signs:
Tremors, warm extremities, tachycardia,
proptosis, goiter etc.
Another sign commonly seen in
hyperthyroidism on the ECG is atrial
fibrillation.
30.
LABORATORY EVALUATION
TSH,FT3,FT4
TRAb
Thyroid ultrasound with doppler flow
Graves’ disease –high blood flow
Postpartum thyroiditid-low blood flow
Radionuclide imaging is contraindicated in
pregnant women
31.
FETAL EFFECTS OFMATERNAL
HYPERTHYROIDISM:
1-5% neonates born to women with Graves’
disease have hyperthyroidism due to
transplacental transfer of TSH-receptor-
stimulating antibodies.
Fetal tachycardia (>160 bpm)
Fetal goiter
Advanced bone age
Craniosynostosis
Cardiac failure
Hydrops
IUGR
32.
MANAGEMENT
1) Thionamides (anti-thyroiddrugs/ ATD).
Act by blocking the production of thyroid hormones
in the thyroid gland.
Propylthiouracil (PTU)=50 mg BD/TDS
Methimazole=10mg OD
2) Beta blockers –to treat tachycardia and tremor
Eg. metoprolol / propranolol
3)Thyroidectomy –rarely used in patients who cannot
tolerate ATD.
Radioactive iodine is contraindicated in pregnancy
33.
TREATMENT NOT REQUIREDIN:
Transient ,subclinical hyperthyroidism
hCG mediated ,overt hyperthyroidism
(gestational transient thyrotoxicosis)
Hyperemesis gravidarum associated
hyperthyroidism
Subclinical and mild asymptomatic overt
hyperthyroidism due to Graves’ disease,
toxic adenoma or toxic multinodular goiter
34.
All theATDs cross the placental barrier and so they may cause
a risk of birth defects during the initial phases of pregnancy
and may also have a potential risk of causing hypothyroidism
in the fetus during the last trimester of pregnancy.
The aim of ATD therapy is to attempt to maintain the range of
thyroid hormones at its upper point of the normal range with
the minimum possible dosages of the drugs.
It is recommended to initiate therapy with PTU during the
first trimester and later shift over to Methimazole during
second trimester of pregnancy.
Liver function tests have to be monitored due to potential
risks of liver failure seen in patients on treatment of
hyperthyroidism with PTU.
The titration of the drug dosages have to be done based on
the FT4 levels and not the TSH as the TSH values take
multiple weeks to return back to its reference range.
35.
POSTPARTUM ISSUES
Breastfeeding mothers:
PTU and methimazole both are generally
excreted in breast milk.
Methimazole is preferred over PTU as PTU is
hepatotoxic
It should be administered following a feeding
in divided doses
Thyroid function test is done after one and
three months in infants.
36.
Management in postpartumpatients of
hyperthyroidism:
Relapse of Graves' disease is seen in a large number
of females within 3 months of their delivery.
This may be due to the disappearance of
Immunosuppression of pregnancy.
TSH and FT4 values need to be monitored at 6
weeks and 12 week interval.
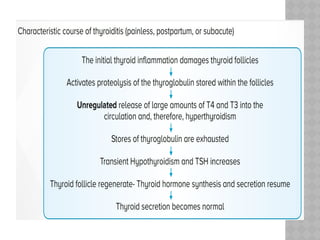
Postpartum thyroiditisis a destructive
thyroiditis induced by an autoimmune
mechanism within one year after parturition.
Postpartum thyroiditis, like painless
thyroiditis, is considered a variant form of
chronic autoimmune thyroiditis (Hashimoto's
thyroiditis)
The prevalence of postpartum thyroiditis
varies globally and ranges from 1 to 17 %.
39.
It occursmore often in women with a previous
history of postpartum thyroiditis, positive
antithyroid peroxidase antibody titers, and type 1
diabetes.
Presentation: It may present in one of the 3 ways:
1. Transient hyperthyroidism alone
2. Transient hypothyroidism alone
3. Transient hyperthyroidism followed by
hypothyroidism and then recovery
Most women recover and are euthyroid within one
year postpartum. However, some women never
recover from the initial hypothyroid phase and have
permanent hypothyroidism or goitre.
41.
CLINICAL MANIFESTATION OFPOSTPARTUM
THYROIDITIS CAN BE VARIABLE
Approximately 20 to 30 percent of women
with
postpartum thyroiditis have the characteristic
sequence of hyperthyroidism, which usually
begins one to four months after delivery and
lasts two to eight weeks, followed by
hypothyroidism,which lasts from
approximately two weeks to six months, and
then recovery
42.
20 to40 percent have only
hyperthyroidism which begins two to six
months after delivery.
Symptoms are typically mild and consist
mainly of fatigue, weight loss, palpitations,
heat intolerance, anxiety,irritability,
tachycardia, and tremor.
43.
Remaining 40to 50 percent have only
hypothyroidism, which begins two to six
months after delivery.
Symptoms are usually mild, leading to lack of
energy, cold intolerance, constipation,
sluggishness, and dry skin.
Some women do not restore normal
endogenous thyroid function after the initial
episode of hypothyroidism.
44.
LABORATORY FINDINGS
Hyperthyroidphase= High or normal free T4
and T3 ,Low TSH
Hypothyroid phase =Low or normal Free T4
and T3 High TSH
45.
DIAGNOSIS
High degreeof clinical suspicion based on
the presenting features and backed up by
laboratory test of thyroid functions form a
base for diagnosis.
Women with hypothyroidism also are prone
to postpartum depression (PPD). It is
therefore prudent to investigate women
presenting with PPD for thyroid disorders.
Drug of choicein hyperthyroidism in pregnancy
in first trimester .
A)Propylthiouracil
B)Methimazole
C)Neomercazole
D)none of the above
Most common cause of hypothyroidism in
pregnancy.
A)Hashimotos’s thyroiditis
B) Iodine deficiency
C)Post thyroidectomy
D)none of the above
49.
Which of thefollowing drug is excreted in breast
milk
A)PTU
B)Methimazole
C)both of the above
D)none of the above
Normal range of TSH in second trimester .
A)0.1-2.5 mIU/L
B)0.1-3 mIU/L
C)0.2-2.5 mIU/L
D)0.2-3 mIU/L


















































![MDR_1st_Dec_2025[1].pptx maternal mortality](https://cdn.slidesharecdn.com/ss_thumbnails/mdr1stdec20251-251203175305-40cf031e-thumbnail.jpg?width=640&height=640&fit=bounds)
![MDR_1st_Dec_2025[1] Final.pptx maternal mortality](https://cdn.slidesharecdn.com/ss_thumbnails/mdr1stdec20251final-251203175141-4e224fe5-thumbnail.jpg?width=640&height=640&fit=bounds)


















![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)








