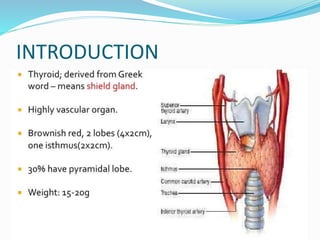
This document discusses thyroid disorders in pregnancy. It notes that hypothyroidism affects 0.05% of pregnant women while hyperthyroidism, mainly Graves' disease, affects 0.05-0.2%. Postpartum thyroiditis occurs in 5-10% of women. The thyroid gland normally enlarges in pregnancy due to increased vascularity. HCG and estrogen levels rise, decreasing TSH and free T4 levels. Treatment aims to maintain euthyroidism. Hyperthyroidism is treated mainly with antithyroid drugs like PTU or carbimazole. Hypothyroidism is treated with levothyroxine. Postpartum thyroiditis can cause transient hyperthyroidism or hyp







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















