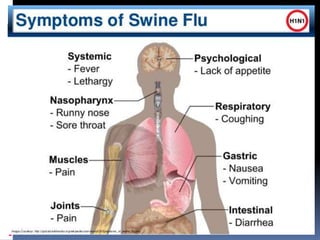
The document discusses Swine Flu in pregnancy. It begins with an introduction defining Swine Flu and noting its spread globally. It then covers the epidemiology of the H1N1 virus, including transmission, incubation period, communicability and seasonality. It defines suspected, probable and confirmed cases and lists populations at highest risk of severe illness, including pregnant women. It discusses potential complications of Swine Flu in pregnancy and recommended investigations, prevention through vaccination, treatment using Oseltamivir, supportive care and discharge policies.


![INTROUCTION
The term “Swine flu” has recently been used
incorrectly to refer to the seasonal influenza A
(H1N1) virus which infects humans.
Influenza A [H1N1], was reported from
Mexico on 18th March, 2009 and rapidly
spread to all the continents.
On June, 2009 the Pakistan health ministry
confirmed the country’s first swine flu case in
a young boy of 14 years old (Dawn News).](https://image.slidesharecdn.com/swinefluinpregnancy-170917130545/85/Swine-flu-in-pregnancy-2-320.jpg)





![Discharge Policy
Patients who have responded to
treatment and are clinically stable - may
be discharged 24 hours of defervesce at
the discretion of attending physician
with total 5 days of Oseltamivir
treatment.
Chemoprophylaxis
It is advised for those contacts who are in
high risk group (with under lying systemic
diseases; extremes of age[<5 years and
65> years]](https://image.slidesharecdn.com/swinefluinpregnancy-170917130545/85/Swine-flu-in-pregnancy-32-320.jpg)






















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

