Downloaded 1,707 times
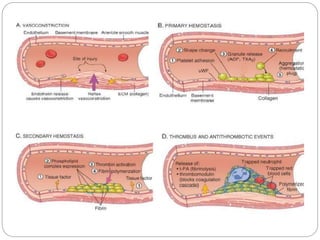
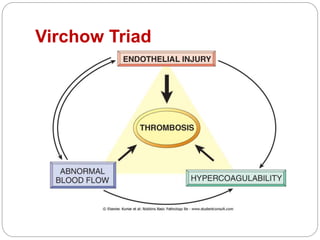
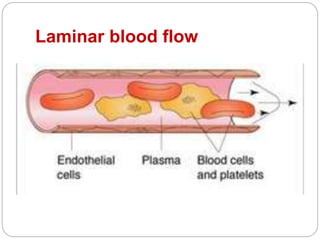
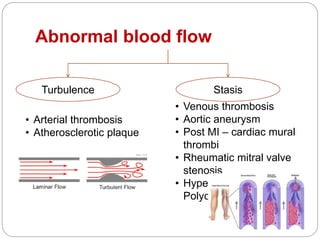
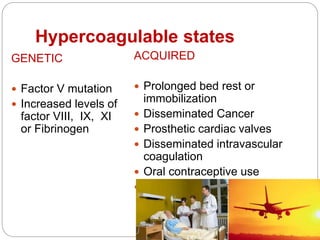
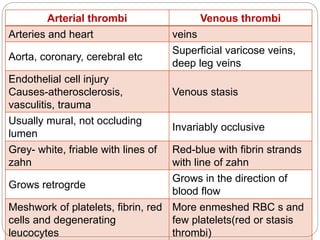
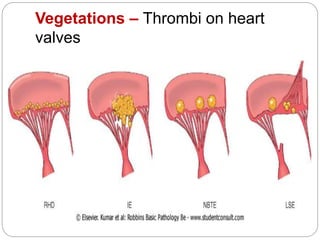
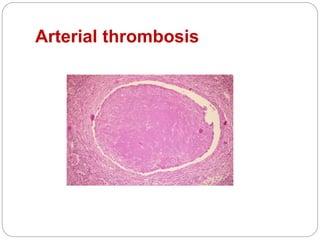
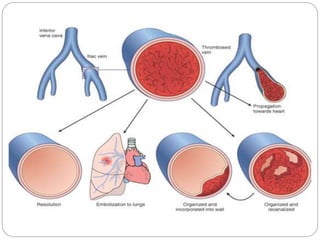

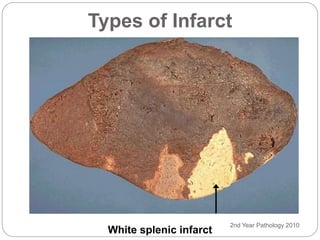

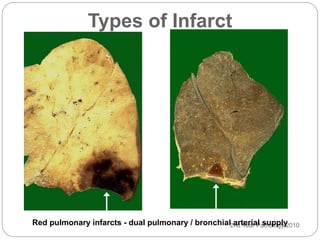
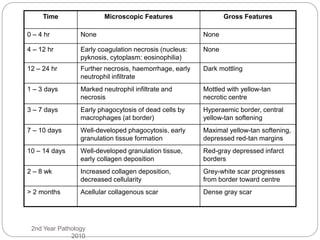


Thrombosis is the formation of a blood clot within a blood vessel or cavity of the heart. Virchow identified three main factors that contribute to thrombosis: endothelial injury, changes in blood flow, and hypercoagulability. Thrombi can propagate or embolize, becoming lodged in another vessel and resulting in infarction of downstream tissue. Infarctions appear pale/white in solid organs and red/hemorrhagic in lungs/other tissues. Over time, infarcted tissue progresses from coagulative necrosis to phagocytosis and scar formation.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








