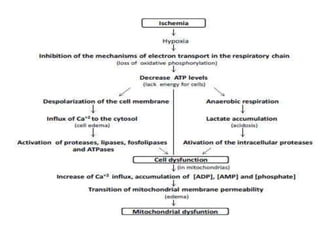
Hemodynamic changes can include hyperaemia, thrombosis, embolism, ischemia, infarction, and hemorrhage. Hyperaemia is increased blood flow to an organ and can be active or passive. Thrombosis is the formation of a blood clot within a blood vessel. Embolism occurs when a detached clot or other mass travels through the bloodstream and blocks a vessel. Ischemia is reduced blood flow to an organ, and infarction is tissue death from a lack of blood flow. Hemorrhage involves bleeding outside of blood vessels.