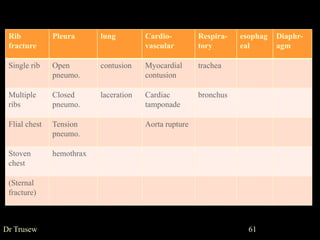
The document discusses various types of thoracic trauma including blunt and penetrating injuries. Immediately life-threatening injuries include tension pneumothorax, massive hemothorax, and flail chest. Rib fractures are common and can range from single fractures to multiple fractures leading to flail chest. Pneumothorax, hemothorax, and tension pneumothorax are discussed in detail. Tension pneumothorax requires urgent needle decompression followed by chest tube placement. Massive hemothorax may require urgent thoracotomy for bleeding control. Clinical assessment focuses on signs of respiratory distress and shock from impaired ventilation or blood loss into the chest cavity.