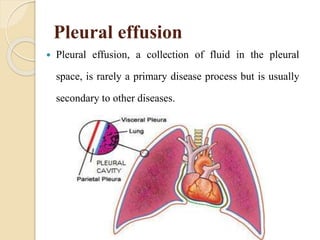
Pleural effusion is an accumulation of fluid in the pleural space that is usually caused by an underlying condition like heart failure, tuberculosis, or cancer. It can cause shortness of breath. Diagnosis involves physical exam, chest x-ray, and thoracentesis to analyze fluid. Treatment focuses on treating the underlying cause as well as draining fluid to relieve symptoms. Nursing care involves monitoring breathing and oxygen levels, treating fever or infection, managing pain and anxiety, and preventing complications.
![Other treatments such as positive expiratory
pressure or PEP therapy (a simple mask and one
way valve system that provides varying amounts of
expiratory resistance [usually 5 to 15 cm H2O])
Continuous or intermittent positive pressure-
breathing (IPPB)](https://image.slidesharecdn.com/pleuraleffusion-181023061750/85/Pleural-effusion-23-320.jpg)