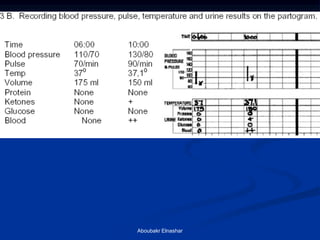

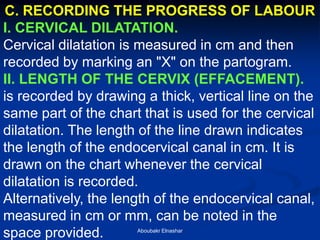
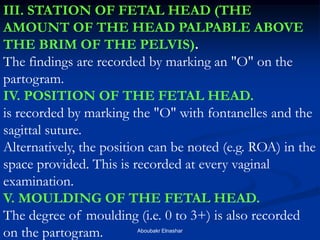
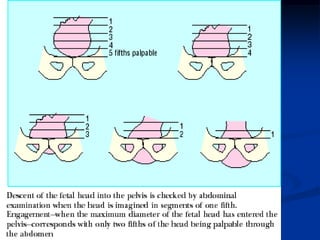
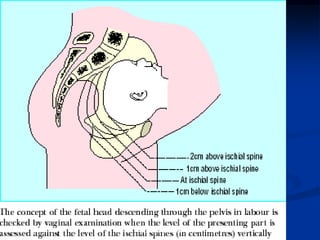



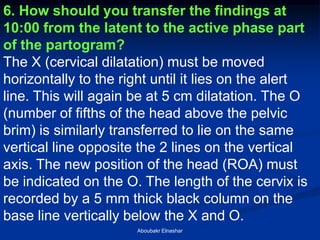
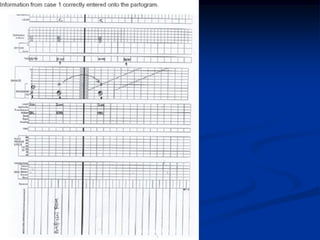
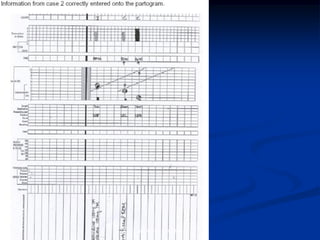
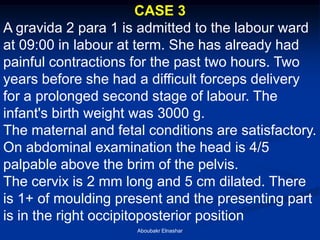
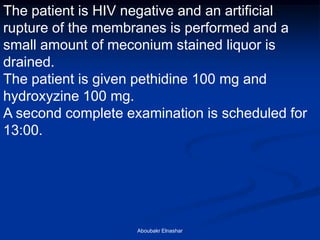
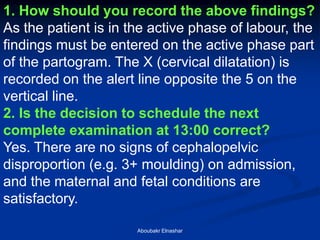
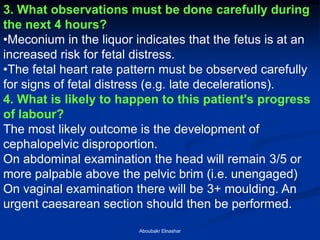
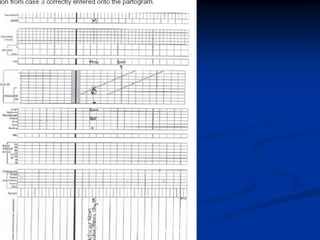
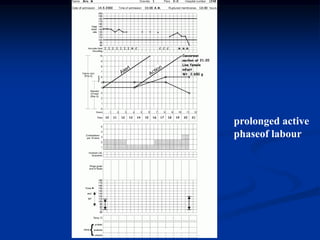
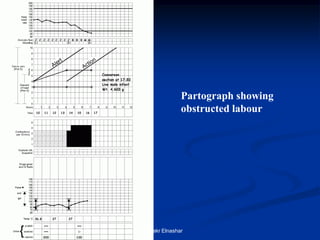
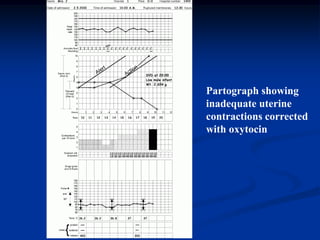

This document provides guidance on how to correctly record information on a partogram, which is used to monitor the progress of labor. It discusses recording the condition of the mother, fetus, and progression of labor through cervical dilation, fetal position, and other metrics. Examples are given of how to record findings from three case studies on the partogram under different scenarios in the latent and active phases of labor, and whether labor is progressing normally or requires additional intervention. The importance of careful monitoring for signs of fetal distress is also emphasized.















































![002 Maintenance M Overview 20 06 06[1]](https://cdn.slidesharecdn.com/ss_thumbnails/002-maintenance-m-overview-20-06-061-1221944333735887-9-thumbnail.jpg?width=640&height=640&fit=bounds)










































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















