Downloaded 178 times
![The Partogram
Dr. C. Savona-Ventura
MD, DScMed, FRCOG, Accr.Cert.OG,
MRCP
The Partogram
• A graphic representation of the progress of
labour
– Cervicograph
– Descent of Head [cf moulding]
– Uterine contractions
– Features that assist progress
[membranes/augmentation/drugs]
– Maternal condition [heart rate, BP, urinalysis]
– Fetal condition [heart rate, liquor]
1](https://image.slidesharecdn.com/partogram-110401040918-phpapp01/85/Partogram-1-320.jpg)
![Phases in progress of Labour
• LATENT PHASE:-
» Nullipara Multipara
» 8.6-20.6 hrs 5.3-13.6 hrs
• ACTIVE PHASE:-
– Acceleration Phase ] 4.9-11.7 hrs 2.2-5.2 hrs
– Phase of Maximum Slope ]
– Deceleration Phase 54 min-3.3 hrs 14 -53 min
• SECOND STAGE 57 min-2.5 hrs 18 -50 min
• THIRD STAGE up to 20 min
Labour progress - cervical
dilatation
10
2nd Stage
8
1st Stage of Labour
6
LATENT 1 cm/hr
4
PHASE ACTIVE
2
PHASE
0
0 5 10 15 20
2](https://image.slidesharecdn.com/partogram-110401040918-phpapp01/85/Partogram-2-320.jpg)
![Latent Phase
• Poor rate of cervical dilatation but general preparation of
cervix.
• Duration: Nullipara Multipara
» 8.6-20.6 hrs 5.3-13.6 hrs
• Assessed using Bishop Score 0 1 2 3
– Cervical dilatation 0 1-2 3-4 5-6+
– Cervical effacement [%] 0-40 40-60 60-80 80+
[cm] 3 2 1 0
– Cervical position Post Mid Ant
– Cervical consistency Firm Mod Soft
– Station re ischial spine [cm] -3 -2 -1,0 +1,+2
• The use of the partogram during the latent phase not of use
since this would chart only cervical dilatation. We should use a
cervicograph.
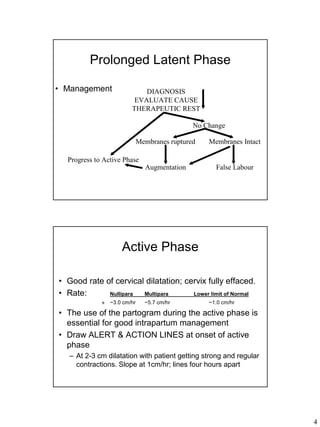
Prolonged Latent Phase
• Definition
– >20 hrs [nullipara]; >14 hrs [multipara]
• Aetiology
– Excessive sedation
– Unfavourable Cervix
– Idiopathic [forced induction]
– False Labour
• Outcome
– 14% will go into a Protracted Active Phase
3](https://image.slidesharecdn.com/partogram-110401040918-phpapp01/85/Partogram-3-320.jpg)
![Descent of head in fifths per
abdomen
• Engagement at 2/5 and less
• If 3/5 or more than CPD [absolute or
relative] is present
Vaginal assessment in
relation to ischial spines not
useful to define engagement
since position of spines
dependant on type of pelvis.
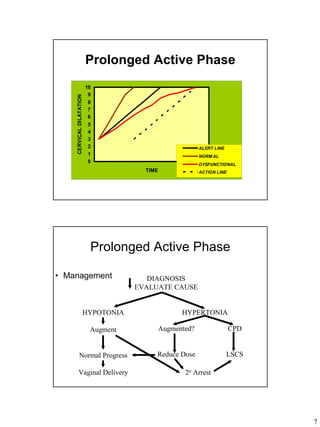
Prolonged Active Phase
• Definition
– >6 hrs or >1.2 cm/hr [nullipara]; >5.2 hrs or >1.5 cm/hr [multipara]
• Aetiology
– CephaloPelvic Disproportion [often relative]
– Fetal head malposition: OP/OT
– Idiopathic [early ARM]
– Excessive sedation
• Outcome
– 39% Po & 13% P1+ will go into Secondary Arrest
6](https://image.slidesharecdn.com/partogram-110401040918-phpapp01/85/Partogram-6-320.jpg)
![Secondary Arrest of Active
Phase
• Definition
– No change in cervical dilatation over a period of 2hrs+. Cervix becomes
oedematous. Can occur at 4-7 cm dilatation or as a protracted Deceleration
phase
• Aetiology
– CephaloPelvic Disproportion [often absolute]
– Fetal head malposition [OP/OT] or Malpresentation [breech]
– Insufficient uterine action
– Excessive sedation
• Outcome
– Will require LSCS. If protracted deceleration beware of shoulder
impaction
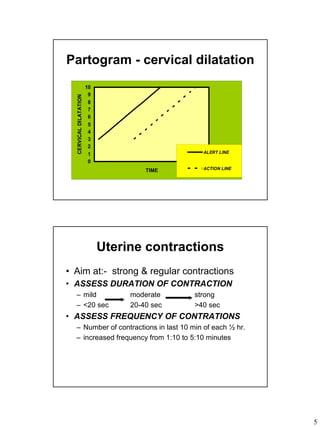
Partogram - cervical dilatation
10
9
CERVICAL DILATATION
8
7
6
5
4
3
2 ALERT LINE
1 NORM AL
0 2 ARREST
PROTRACTED
TIME ACTION LINE
8](https://image.slidesharecdn.com/partogram-110401040918-phpapp01/85/Partogram-8-320.jpg)


The document discusses the use of the partogram to monitor labor progress. It describes the phases of labor including the latent phase, active phase, second stage, and third stage. It provides details on normal durations and cervical dilation rates. The partogram is useful for charting cervical dilation, contractions, descent of the fetal head, and identifying prolonged or abnormal labor that may require interventions like augmentation or C-section. Prolonged phases can be caused by issues like CPD, fetal malposition, or insufficient contractions.










































































































