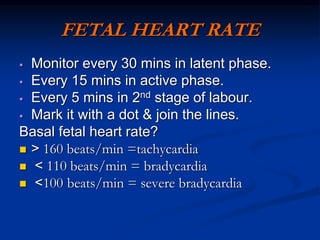
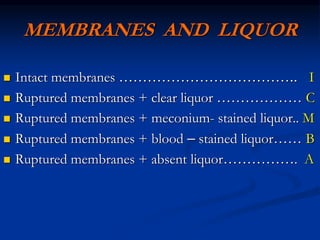
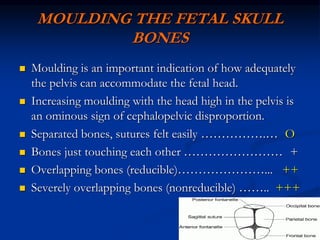
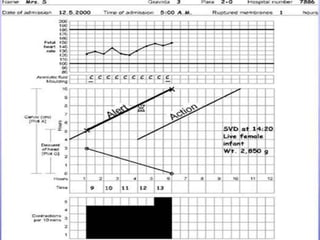
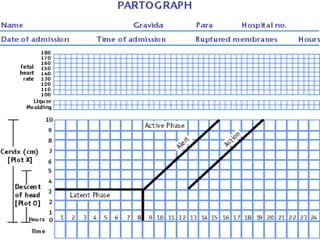
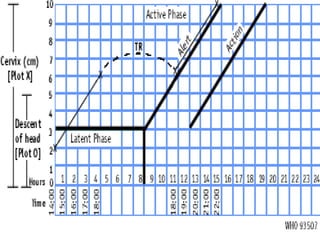
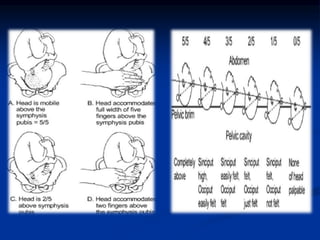
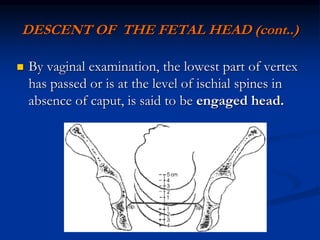
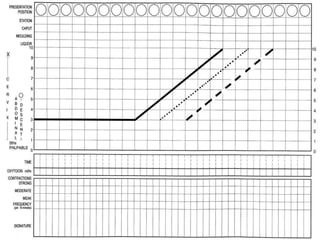
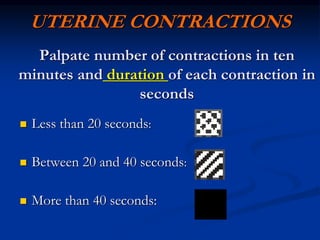
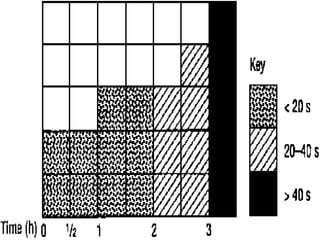
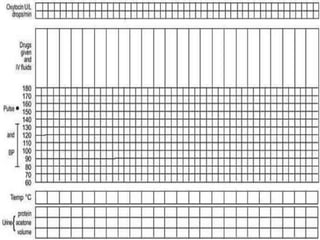
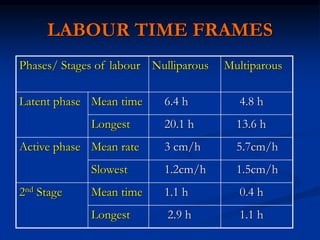
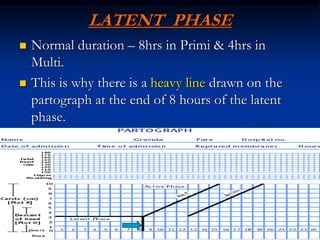
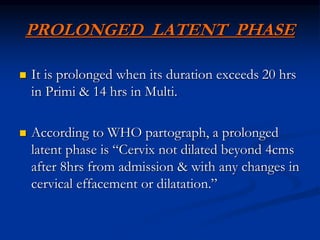
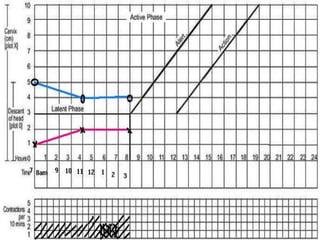
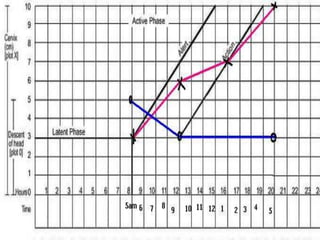
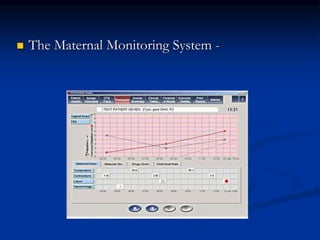
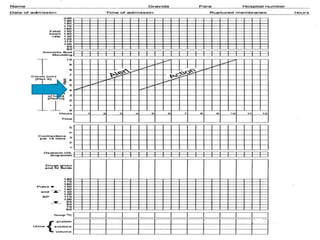
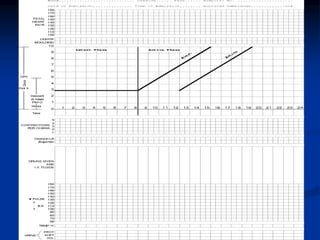
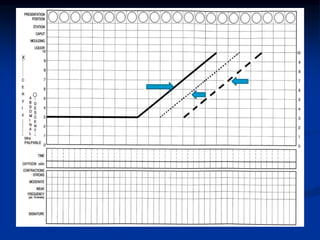
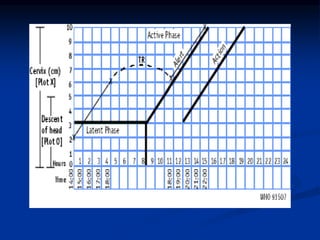
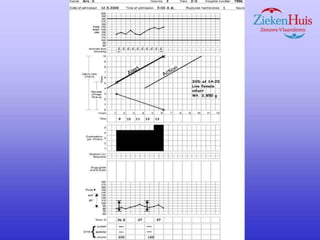
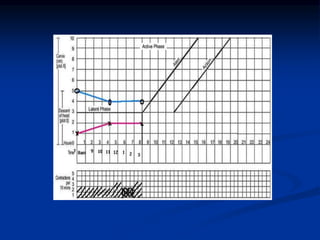
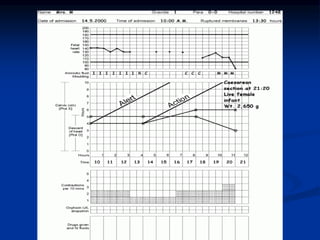
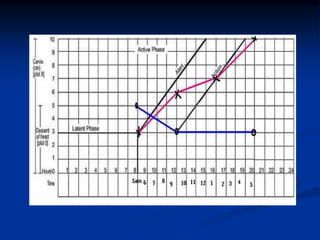
The document provides information on using a partograph to monitor labor. A partograph is a composite chart used to graphically record observations of a woman in labor. It can serve as an early warning system to detect abnormal labor progress and help make timely decisions about interventions. Key components of the partograph include monitoring cervical dilation, fetal descent, contractions, and maternal condition. Deviations from normal labor progress such as a prolonged latent phase or active phase may indicate issues that require actions like transfer or augmentation of labor.













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















