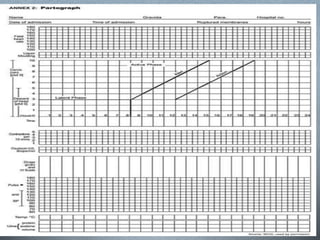
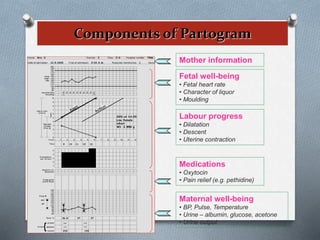
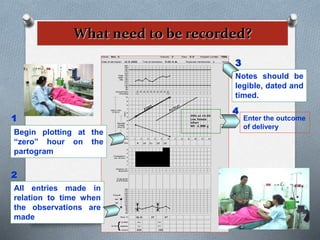
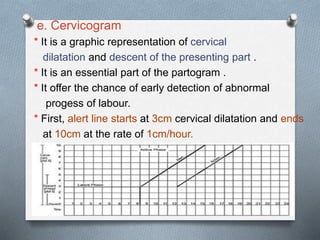
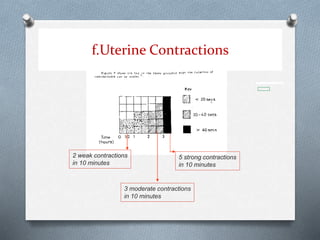
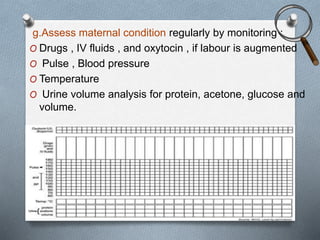
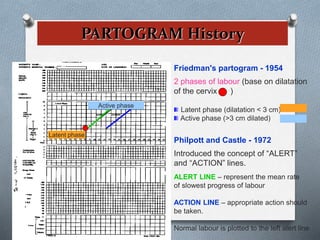
This document discusses the partograph, which is a composite graphical record used to monitor labor. It is used to assess the progress of normal and abnormal labor and the fetal response. The partograph allows providers to visualize cervical dilation over time and identify issues early. It includes components like maternal information, fetal well-being, labor progress, medications, and maternal condition. Using a partograph has benefits like early detection of problems, prevention of prolonged labor, and improved outcomes for mothers and babies.

















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

