Download as PDF, PPTX






![TeLinde's Modification of the American Fertility
Society Classification of Uterovaginal Anomalies[3]
Class I. Dysgenesis of the Mullerian Ducts
Class II. Disorders of Vertical Fusion of the Mullerian Ducts
Class III. Disorders of Lateral Fusion of the Mullerian Ducts
Class IV. Unusual Configuration of Vertical-Lateral Fusion Defects
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/utanomalies-150628015506-lva1-app6891/85/MULLERIAN-DUCT-ANOMALIES-45-320.jpg)

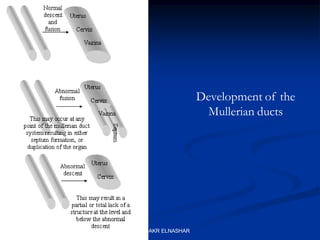
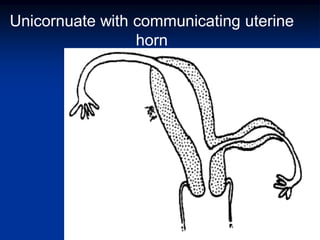
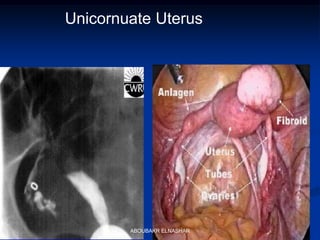
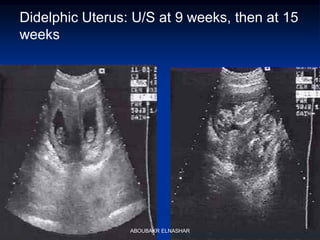
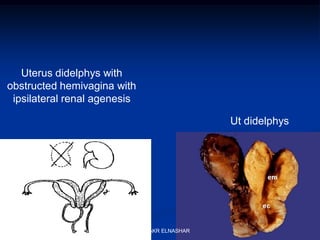
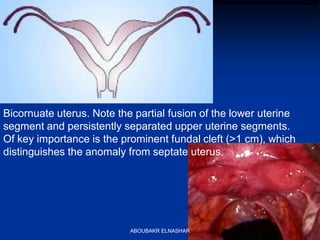
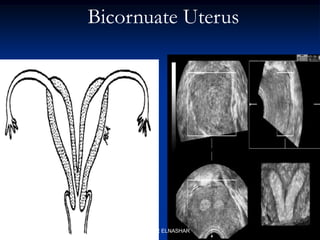
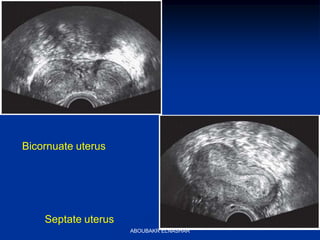
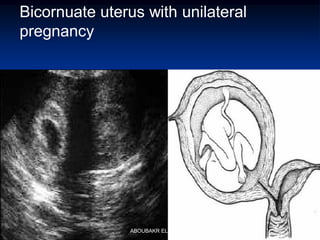
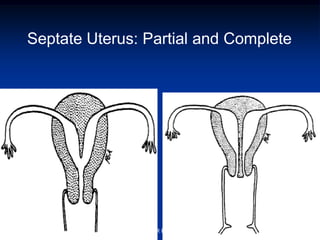
1. The müllerian ducts normally develop into the fallopian tubes, uterus, cervix, and upper two-thirds of the vagina. Failures or abnormalities during development can result in müllerian duct anomalies. 2. Development occurs through three phases - organogenesis, fusion, and septal resorption. Failures in fusion can lead to bicornuate or didelphys uterus, while failed septal resorption causes septate uterus. 3. Müllerian duct anomalies have a variety of presentations including infertility, miscarriage, and obstructed reproductive systems. Diagnosis is made through ultrasound, hysterosalpingography, or laparoscopy.







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















