Download as PDF, PPTX
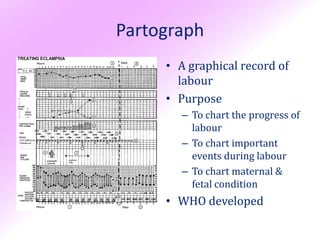



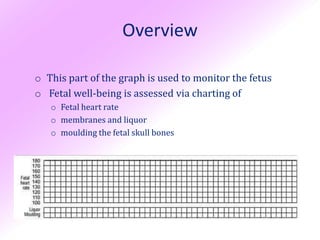

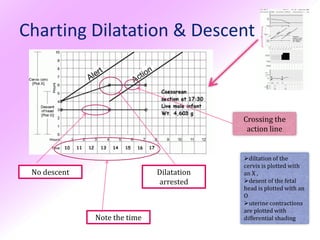

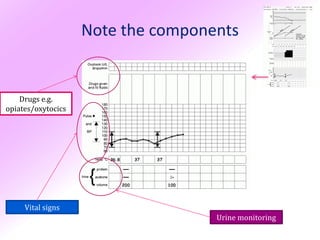

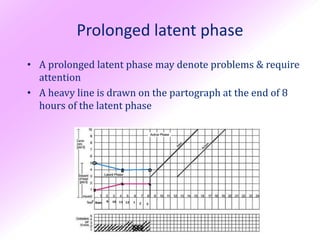
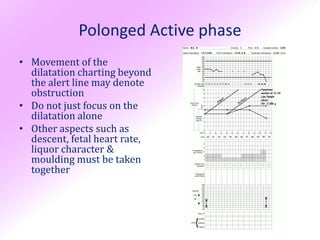
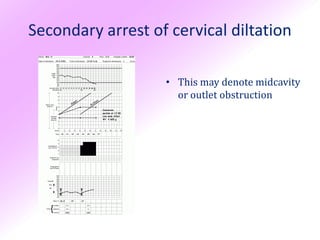
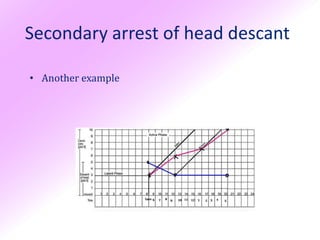

1) The partograph is a graphical record used to monitor the progress of labour and detect abnormalities through charting cervical dilation, fetal descent, contractions, and fetal/maternal conditions. 2) It consists of 3 sections - fetal condition, labour progress, and maternal condition - to provide an objective assessment of factors indicating normal vs obstructed labour. 3) Abnormal progress detected by crossing the alert line (1cm dilation/hour) or action line requires reassessment and management decisions to prevent complications.






































































































