Downloaded 881 times













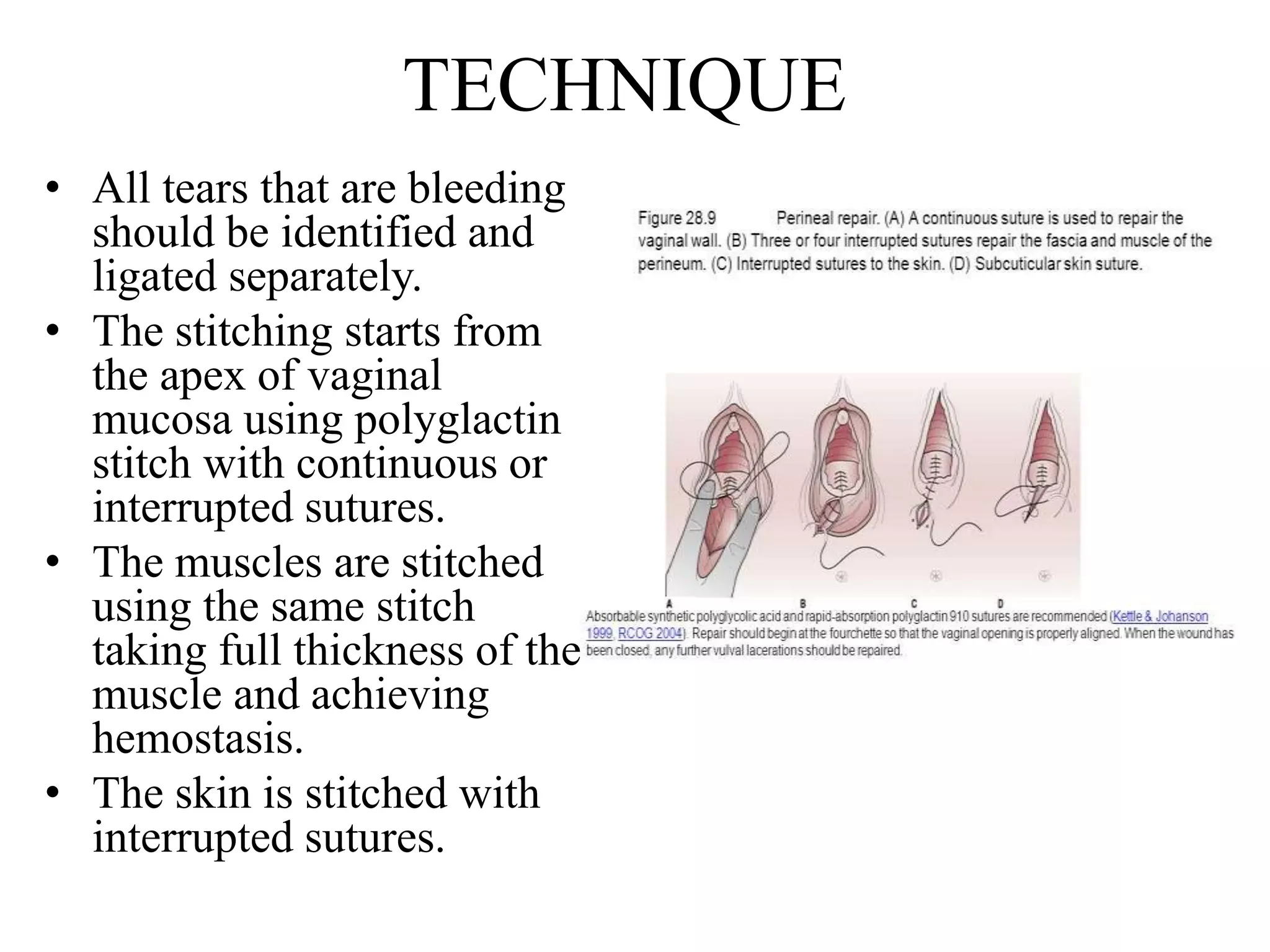




















This case report describes a 20-year-old woman who experienced a third degree perineal tear and cervical tear during her vaginal delivery. She underwent repair of the tears which involved suturing the anal mucosa, external and internal sphincters, and left side of the cervix. Her post-operative recovery included antibiotics, sitz baths, and pelvic floor exercises. Perineal tears can occur due to obstetric factors like prolonged labor or operative delivery, and non-obstetric injuries. They are classified based on the extent of tissue involvement and proper identification and repair is important for recovery.



































































