Download to read offline
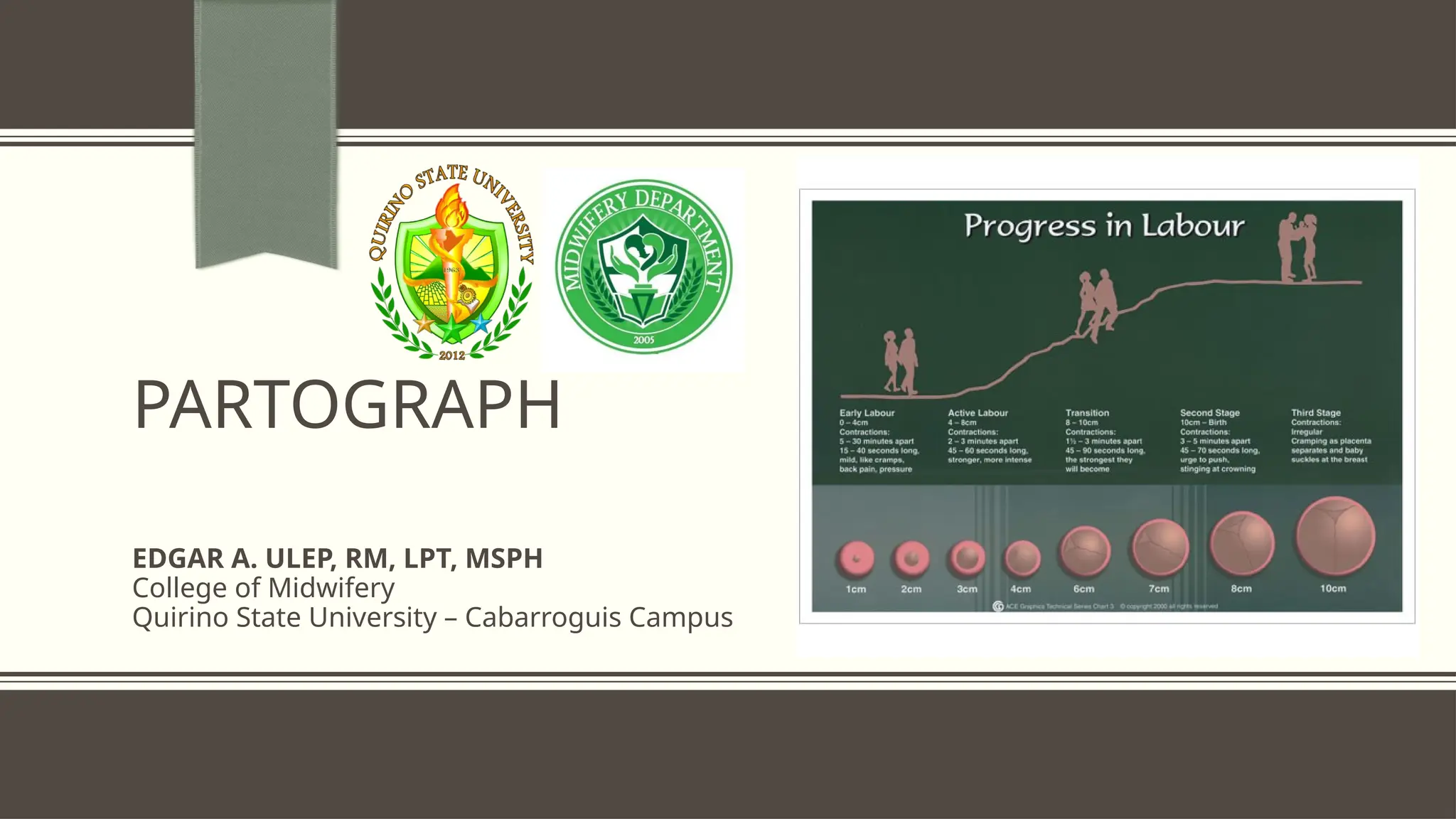













The document discusses the partograph, a graphical tool for recording cervical dilatation and fetal and maternal conditions during labor. It outlines its history, advantages, principles of plotting, and methods of recording key information about labor. Specific guidelines for monitoring labor progress and conditions warranting use or non-use of the partograph are also provided.























































