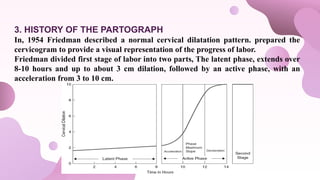
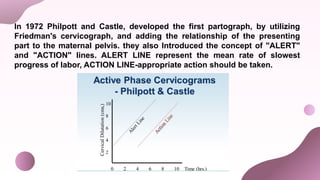
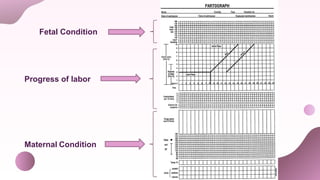
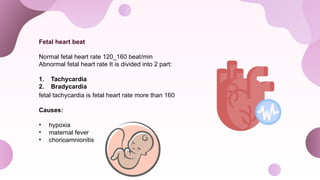
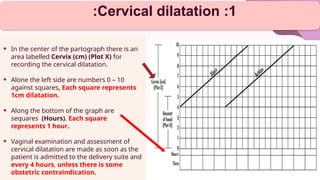
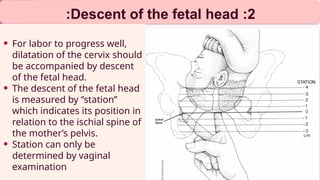
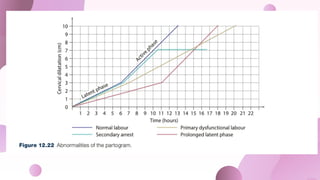
The document discusses the partogram, a vital tool in obstetric care for tracking labor progress and maternal and fetal conditions, introduced in the 1970s. It highlights components such as monitoring vital signs, fetal heart rates, and cervical dilation while emphasizing its role in early detection of complications. Despite its advantages for decision-making and safety, the partogram has limitations, including subjective assessments and cultural barriers.





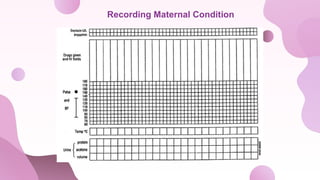
![Recording Maternal Condition
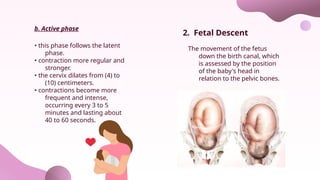
All observation for
the mother’s
condition is written at
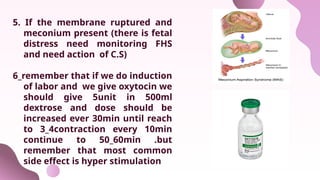
the bottom of the
paragraph
Recording the
condition of mother :
mother’s
information
Name, age, date
&time of admission,
gravidity and parity ,
time of rupture
membrane.
Medications
-Oxytocin drip (if
labour augmented )
Oxytocin unit per
volume IV fluids
[ oxytocin U/L ] in
drops per minute
[ drops/min ] every 30
minutes
-Drugs and other
intravenous
fluids(if used)
Includes: analgesic
(pain relief e.g
pethidine),
antibiotics ,etc…
Should be written
the name of drug &
dose in the long
box at the particle
point of time.](https://image.slidesharecdn.com/partogram22-241013104152-385372de/85/Partogram-Partogram-Partogram-Partogram-18-320.jpg)
![Vital sings
Assess maternal
condition regularly by By
repeat the monitoring
her pulse ,Bp, and
temprture.
-pulse : should be
checked every half to 1
hour and marked with a
dot [ • ]
-Blood pressure :
measured every 4 hours
and marked with arrows
[ ] if high risk case,
should be measured
more frequent time every
half to 1 hour.
Urine volume ,analysis
for patien & acetone
During course of labour ,
checking hydration by
volume of urine , and
check urine sample
looked for proteins &
ketone , is absent marked
by [ _ ]
In case of maternal
distress the volume may
be decreased.
-Temperature: recorded every 4
hours.](https://image.slidesharecdn.com/partogram22-241013104152-385372de/85/Partogram-Partogram-Partogram-Partogram-19-320.jpg)







2.Friedman, E. A. (1954). "Labor and Delivery." American Journal of Obstetrics and Gynecology.
3.Philpott, R. H., & Castle, W. M. (1972). "The Partograph: A New Tool for the Management of
Labor." Journal of Obstetrics and Gynaecology.
4.Roberts, J. A., & Morrison, J. (2020). Textbook of Obstetrics. 3rd Edition. Elsevier.
5.Wikipedia. "Partogram." Available at: [Wikipedia Partogram
Page](https://en.wikipedia.org/wiki/Partogram)
6.Khan, K. N., et al. (2016). "The Use of Partogram in Labor Management: A Review." International
Journal of Obstetric Anesthesia, 25(2), 89-94.
7.Madhuri, R. M., et al. (2017). "Evaluation of Partogram in the Management of Labor." Journal of
Clinical and Diagnostic Research, 11(7), QC05-QC08.
8.Choudhury, R., & Singh, R. (2019). "Role of Partograph in Labor Management: A Review." Journal
of Obstetrics and Gynaecology, 39(4), 477-481.](https://image.slidesharecdn.com/partogram22-241013104152-385372de/85/Partogram-Partogram-Partogram-Partogram-49-320.jpg)