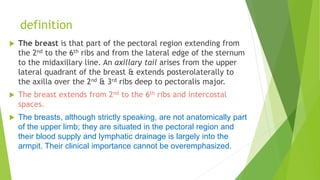
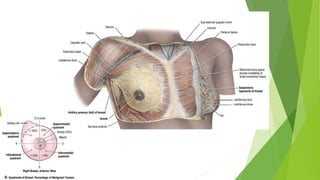
The breast extends from the 2nd to 6th ribs and consists of 15-20 lobes that radiate out from the nipple. Each lobe contains ducts that open on the nipple and deliver milk. The breasts develop during puberty under the influence of hormones and further enlarge during pregnancy as the ducts and milk-producing alveoli grow. Lymph drains from the breasts to axillary and internal thoracic lymph nodes, and the breasts receive blood supply from intercostal and thoracoacromial arteries.










































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















