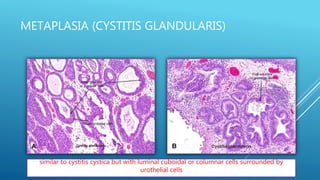
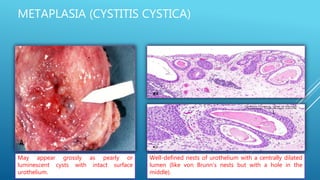
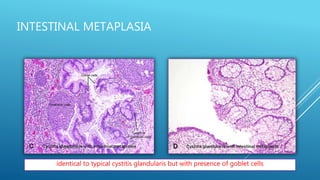
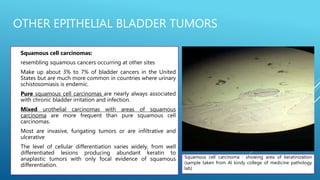
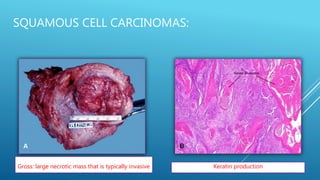
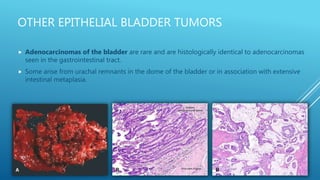
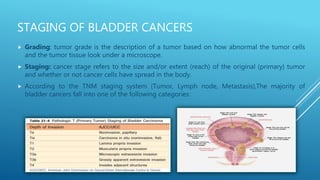
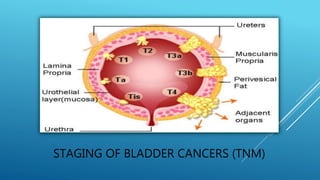
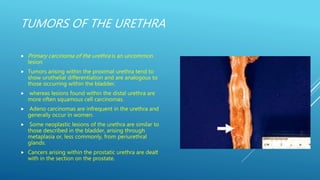
This document discusses various pathologies of the ureter, bladder, and urethra. It begins by describing common congenital anomalies of the ureter including double and bifid ureters as well as ureteropelvic junction obstruction. It then discusses non-neoplastic conditions of the bladder such as vesical diverticula, cystitis, and various metaplastic lesions. Neoplastic conditions covered include urothelial carcinoma and adenocarcinomas of the bladder. Finally, it briefly mentions primary carcinoma of the urethra.

















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









