INTRODUCTION
• The breastor the mamma is the modified sweat gland and lies un the
superficial fascia of pectoral region, and has no distinct fibrous
capsule.
• The breast are present bilaterally in the pectoral region of both the
sexes.
• In males and females, in non reproductive age group, the breast are
present as rudimentary structures. Nipples and small but the areola is
fully formed.
• The shape varies in adult females, which may be hemispherical,
conical or pendulous; but its circular base remains fairly constant.
3.
• After puberty,the female breast becomes well developed.
• Breast development is the most important secondary sexual character
and is caused due to action of estrogen during puberty. Later on the
breast development is due to the action of estrogen and progesterone.
• During puberty breast development happens in 5 stages.
4.
FEMALE BREAST
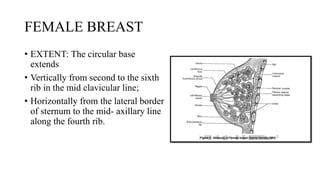
• EXTENT:The circular base
extends
• Vertically from second to the sixth
rib in the mid clavicular line;
• Horizontally from the lateral border
of sternum to the mid- axillary line
along the fourth rib.
5.
• Mammary bed:The base of the glands rest upon the following structures:
• Pectoralis major muscle, in the medial two- thirds;
• Serratus anterior muscle ;, in lateral one- third;
• External oblique aponeurosis in the infero-medial quadrant.
• Retro-mammary space- contains loose connective tissue intervenes between
the base of the gland and the deep fascia covering the structures of the
mammary bed. Due to this arrangement of the breast over pectoralis major
muscle normal breasts are freely movable.
• In invasive breast cancer the glands become fixed on pectoralis major
muscle.
6.
• Axillary tailof spence: sometimes a tail like projection from the upper
and outer quadrant of the gland enters the axilla through an opening on
the axillary fascia known as foramen of Langer.
7.
EXTERNAL FEATURES OFFEMALE
BREAST
NIPPLE:
• It is a conical or cylindrical projection below the center of the breast,
at the level of fourth intercostal space in nulliparous females.
• The nipple id pierced by 15- 20 lactiferous ducts, and contains circular
and longitudinally arranged smooth muscles. The circular muscle
erects the nipple for suckling; the longitudinal muscle retracts the
nipple.
• Nipple is richly supplied by the nerves and is provided with the
sensory receptors for suckling.
8.
AREOLA:
• It isthe pigmented circular area of the skin around the base of the
nipple.
• During pregnancy the areola becomes irreversibly darkened and the
outer margins of the areola contains a number of modified sebaceous
gland, which are enlarged during pregnancy and the lactation known
as the tubercles of Montgomery; oily secretions provide protective
lubricant during lactation.
• Areola also contains sweat glands and accessory mammary glands and
the skin is devoid of hair and subcutaneous fat.
9.
MALE BREAST
• Itis essentially composed of duct system without alveoli and is
supported by fibro-fatty tissue. The breast tissue does not extend
beyond the margin of areola.
• Abnormal and bilateral hypertrophy of male breast (gynaecomastia)
are occasionally observed in Klinefelter’s syndrome (genotypically,
47, XXY), endocrine disorders or impaired liver function.
• Male breasts are richly drained by lymphatics. Hence the prognosis of
breast carcinoma of male is worse than that of female.
10.
STRUCTURE OF BREAST
1.Glandular tissue:
• Arranged in lobes
• Contains 15- 20 pyramidal lobes, each being drained
by separate lactiferous ducts. The ducts are arranged
in radiating manner and converge towards the areola,
where each duct dilates to form the lactiferous sinus
possibly to act as reservoir of milk; finally the ducts
open on to the nipple.
• Each duct drains a segmental system of smaller ducts
and lobules. Each segmental duct divides into a
number of terminal ducts; from the latter numerous
secretory glands pouch out of form grape- like
clusters.
11.
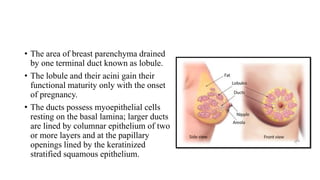
• The areaof breast parenchyma drained
by one terminal duct known as lobule.
• The lobule and their acini gain their
functional maturity only with the onset
of pregnancy.
• The ducts possess myoepithelial cells
resting on the basal lamina; larger ducts
are lined by columnar epithelium of two
or more layers and at the papillary
openings lined by the keratinized
stratified squamous epithelium.
12.
• The carcinomaof breast usually arises from the larger ductal
epithelium.
• Benign fibro-adenoma arise from the smaller ducts. Since these are
freely movable they are also called “breast mouse”
13.
2. Interlobular fattytissue:
• Makes the breast rounded in contour.
• Fat is absent below nipple and areola.
3. Fibrous tissue:
• Supports the lobes and forms a number of septa which anchor the
parenchyma to the overlying skin and the underlying pectoral fascia.
• These fibrous bands are known as suspensory ligaments of Cooper.
• In case of malignant tumors in breast, the cancer may extend along the
ligaments of Cooper and cause dimpling over the skin or fixation of lump
over pectoralis major muscle.
14.
STRUCTURAL DIFFERENTIATION
• Frombirth to pre- puberty there is only presence of lactiferous ducts
without alveoli.
• At puberty; the ducts undergo branching and the peripheral branches
form solid, spheroid mass of cells which are precursors of alveoli.
• In pregnancy; during this period further proliferation and epithelial
growth of terminal ducts and lobules take place with increase in
number of alveoli per lobule. After about 6 months of pregnancy the
size of the breast further increases due to increased blood flow.
• The secreting alveoli expands with accumulation if milk which is
secreted during the later part of pregnancy and few days after
parturition; known as colostrum.
15.
• Colostrum isrich in fats and colostrum corpuscles.
• During lactation; the distended alveoli are lined by single layer of
epithelium, which is separated from the basement membrane by
myoepithelium.
• After lactation; when lactation stops the alveoli shrinks and the
remaining milk is absorbed and the glandular tissue returns to the
resting condition.
16.
Hormones acting onglandular tissue
• Estrogen- stimulates the growth and branching of the ducts;
• Progesterone- stimulates the alveolar formation at the end of the branching
ducts;
• Estrogen and progesterone- placental hormones stimulate the formation of
secretory alveoli during pregnancy.
• Prolactin and growth hormone- maintain lactation
• Oxytocin- helps milk ejection initiated by ejection reflex;
• Maternal estrogen- circulating in neonates of both sexes through the
placenta, stimulates the ductal epithelium of their breast causing transient
hyperplasia to secrete fat free fluid in the first one or two weeks after birth
known as witch’s milk.
17.
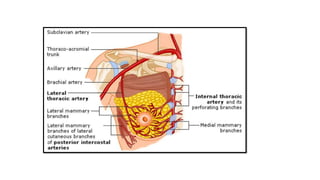
ARTERIAL SUPPLY OFBREAST
1. Lateral thoracic branch of axillary artery provides the lateral
mammary branches, which wind round the pectoralis major and
supply the lateral part of the gland.
2. Superior thoracic artery from the first part of axillary, supplies
upper part of the gland.
3. Perforating branch of internal thoracic artery to the 2nd, 3rd and
4th intercostal spaces form the medial mammary branches, which
supple the medial part of the breast.
4. Lateral branches of 2nd, 3rd and 4th intercostal arteries supply
the deep surface of the gland.
19.
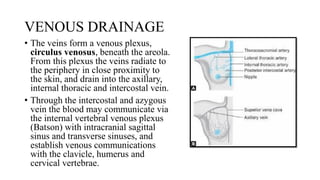
VENOUS DRAINAGE
• Theveins form a venous plexus,
circulus venosus, beneath the areola.
From this plexus the veins radiate to
the periphery in close proximity to
the skin, and drain into the axillary,
internal thoracic and intercostal vein.
• Through the intercostal and azygous
vein the blood may communicate via
the internal vertebral venous plexus
(Batson) with intracranial sagittal
sinus and transverse sinuses, and
establish venous communications
with the clavicle, humerus and
cervical vertebrae.
20.
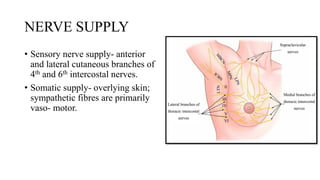
NERVE SUPPLY
• Sensorynerve supply- anterior
and lateral cutaneous branches of
4th and 6th intercostal nerves.
• Somatic supply- overlying skin;
sympathetic fibres are primarily
vaso- motor.
21.
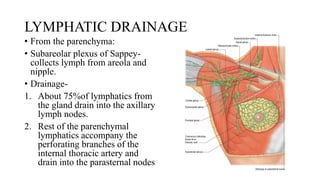
LYMPHATIC DRAINAGE
• Fromthe parenchyma:
• Subareolar plexus of Sappey-
collects lymph from areola and
nipple.
• Drainage-
1. About 75%of lymphatics from
the gland drain into the axillary
lymph nodes.
2. Rest of the parenchymal
lymphatics accompany the
perforating branches of the
internal thoracic artery and
drain into the parasternal nodes
22.
3. About 5%of the lymphatics from the lateral and posterior parts of the
gland follow the posterior intercostal vessels and drain into the posterior
intercostal nodes.
From the overlying skin
1. From the outer part- axillary lymph nodes;
2. From the upper part- supra- clavicular group of lower deep cervical
lymph nodes. Some vessels reach the cephalic nodes in delto pectoral
triangle and then drain into the apical group of axillary lymph nodes.
3. From the inner part- parasternal nodes
23.
• The cutaneouslymphatics communicate across the middle line with
those of the opposite side breast; making the unilateral disease
bilateral by this route.
4. From the lower part- the lymphatics communicate with the rectus
sheath and form a sub-peritoneal plexus. The vessels drain into sub-
diaphragmatic nodes and some drain into hepatic node.
• Enlargement of these nodes during metastatic spread may produce
obstructive jaundice.
• Rarely the cancer cells from the sub-peritoneal plexus undergo
transcoelomic migration and produce secondary deposits on the
ovarian surface forming Krukenberg’s tumour.
24.
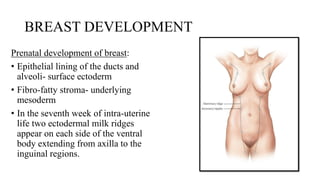
BREAST DEVELOPMENT
Prenatal developmentof breast:
• Epithelial lining of the ducts and
alveoli- surface ectoderm
• Fibro-fatty stroma- underlying
mesoderm
• In the seventh week of intra-uterine
life two ectodermal milk ridges
appear on each side of the ventral
body extending from axilla to the
inguinal regions.
25.
• The pectoralportion if the ridge presents a surface depression,
mammary pits, from the bottom of which about 15 to 20 epithelial
cords grow into underlying dermis. The cords are canalised by the end
of foetal life.
• Shortly before birth the pit evaginates by the growth of underlying
mesoderm and forms nipple.
• The areola becomes apparent during the fifth month on foetal life.
26.
• Mammary linesin humans are visible by day 37
• Invagination of mammary pits- by day 49
• Beginning of nipple formation- day 56
• Sprouting of the primitive ducts- day 84
• Canalisation- day 150
27.
POST NATAL DEVELOPMENT
•From puberty the breast development takes place in females by branching
of the ducts and lobule formation from the terminal ducts.
• Post pubertal growth of female breast or thelarche is classified
chronologically into five stages also called Tanner’s staging.
1. Phase 1- elevation of nipple
2. Phase 2- nipple and subareolar glandular breast tissue project forward as a
single mass
3. Phase 3- breast becomes palpable with increased diameter and
pigmentation of areola
4. Phase 4- nipple are areola form separate projectile mass in front of the
main breast tissue
5. Phase 5- smooth contour of hemispherical breast with fat deposition.
28.
TANNER’S STAGING
• Totalstages of breast and pubic hair development are 5.
• Stage 1 and 2 are early stages of breast development
• Stages 4 and 5 are the later stages of breast development.
29.
CLINICAL ASPECTS
Clinical sign:
•Dimpling – due to involvement of ligament of cooper in malignancy
breasts may show dimpling but is not a sign of skin involvement.
• Retraction of nipple- caused due to fibrosis of lactiferous ducts.
• Peau d’orange- orange peel appearance of the skin over breast due to
sub-dermal/ cutaneous lymphatics involvement. It is caused due to
lymphatic edema of skin and hair follicles.
30.
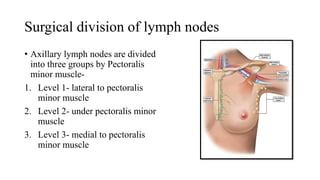
Surgical division oflymph nodes
• Axillary lymph nodes are divided
into three groups by Pectoralis
minor muscle-
1. Level 1- lateral to pectoralis
minor muscle
2. Level 2- under pectoralis minor
muscle
3. Level 3- medial to pectoralis
minor muscle
31.
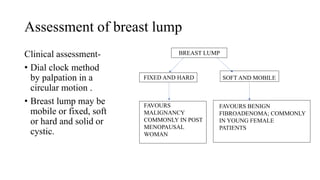
Assessment of breastlump
Clinical assessment-
• Dial clock method
by palpation in a
circular motion .
• Breast lump may be
mobile or fixed, soft
or hard and solid or
cystic.
BREAST LUMP
FIXED AND HARD SOFT AND MOBILE
FAVOURS
MALIGNANCY
COMMONLY IN POST
MENOPAUSAL
WOMAN
FAVOURS BENIGN
FIBROADENOMA; COMMONLY
IN YOUNG FEMALE
PATIENTS
32.
TREATMENT MODALITIES:
1. Surgicalmanagement :
• Breast conservation surgery- lump is surgically excised and is
followed by radiotherapy
• Mastectomy – surgical removal of entire breast and nipple areola
complex.
2. Chemotherapy
3. Radiotherapy
4. Hormonal therapy
33.
References :
• Essentialsof human anatomy by A K Dutta, 4th edition
• Bailey and Love’s short practice of surgery, 27th edition
• A manual on clinical surgery by S Das, 17th edition
• Textbook of gynaecology by D C Dutta , 8th edition