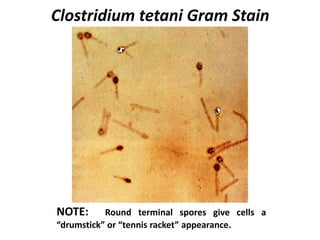
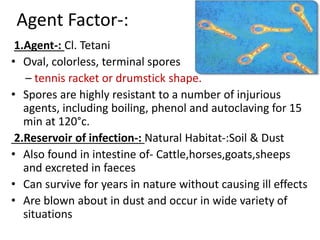
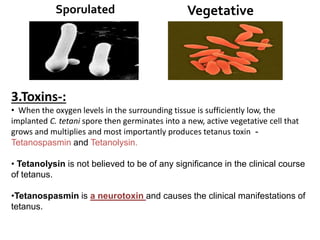
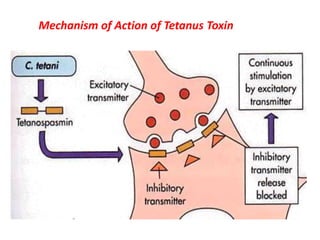
Tetanus is caused by Clostridium tetani bacteria, whose spores are found worldwide in soil. The bacteria produces a neurotoxin called tetanospasmin that causes painful muscle contractions. Tetanus is transmitted through puncture wounds, burns, and other injuries that provide a route of entry for spores. The disease is entirely preventable through active immunization with tetanus toxoid vaccines as part of routine childhood immunization schedules and during pregnancy to prevent neonatal tetanus. Passive immunization with tetanus immunoglobulin provides temporary protection.