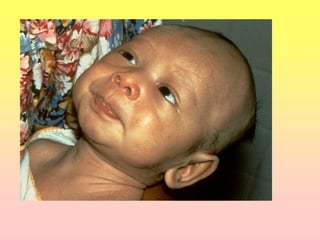
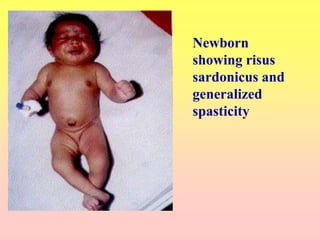
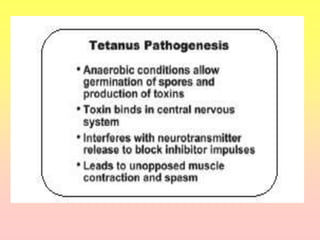
Tetanus is a disease caused by Clostridium tetani bacteria that produces a neurotoxin. It causes muscle spasms and stiffness. The neurotoxin is known as tetanospasmin. Tetanus is characterized by lockjaw and painful muscle spasms. It is prevented through active immunization with tetanus toxoid vaccines. Tetanus spores are found worldwide in soil and animal feces. People become infected through wounds that contain the spores. While not contagious, it has a high fatality rate if not properly treated.