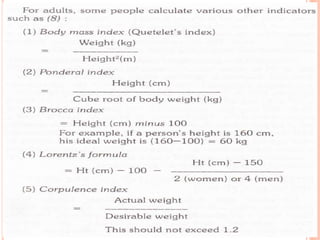
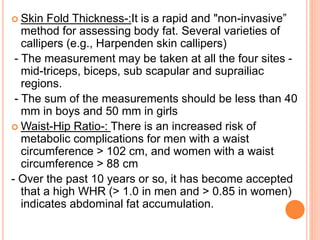
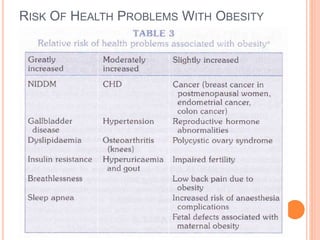
The document discusses obesity as a chronic disease characterized by abnormal fat tissue growth, measured by body mass index (BMI), and affecting various demographics globally. It outlines the epidemiological determinants of obesity including age, sex, genetic factors, physical inactivity, and socio-economic status, alongside methods for obesity assessment such as skin fold thickness and waist-hip ratio. The document concludes with the hazards of obesity, including increased morbidity and mortality, and methods for prevention and control through dietary changes, physical activity, and surgical treatments.































![Obesity by bijay [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/obesitybybijayautosaved-200407031519-thumbnail.jpg?width=640&height=640&fit=bounds)














































