


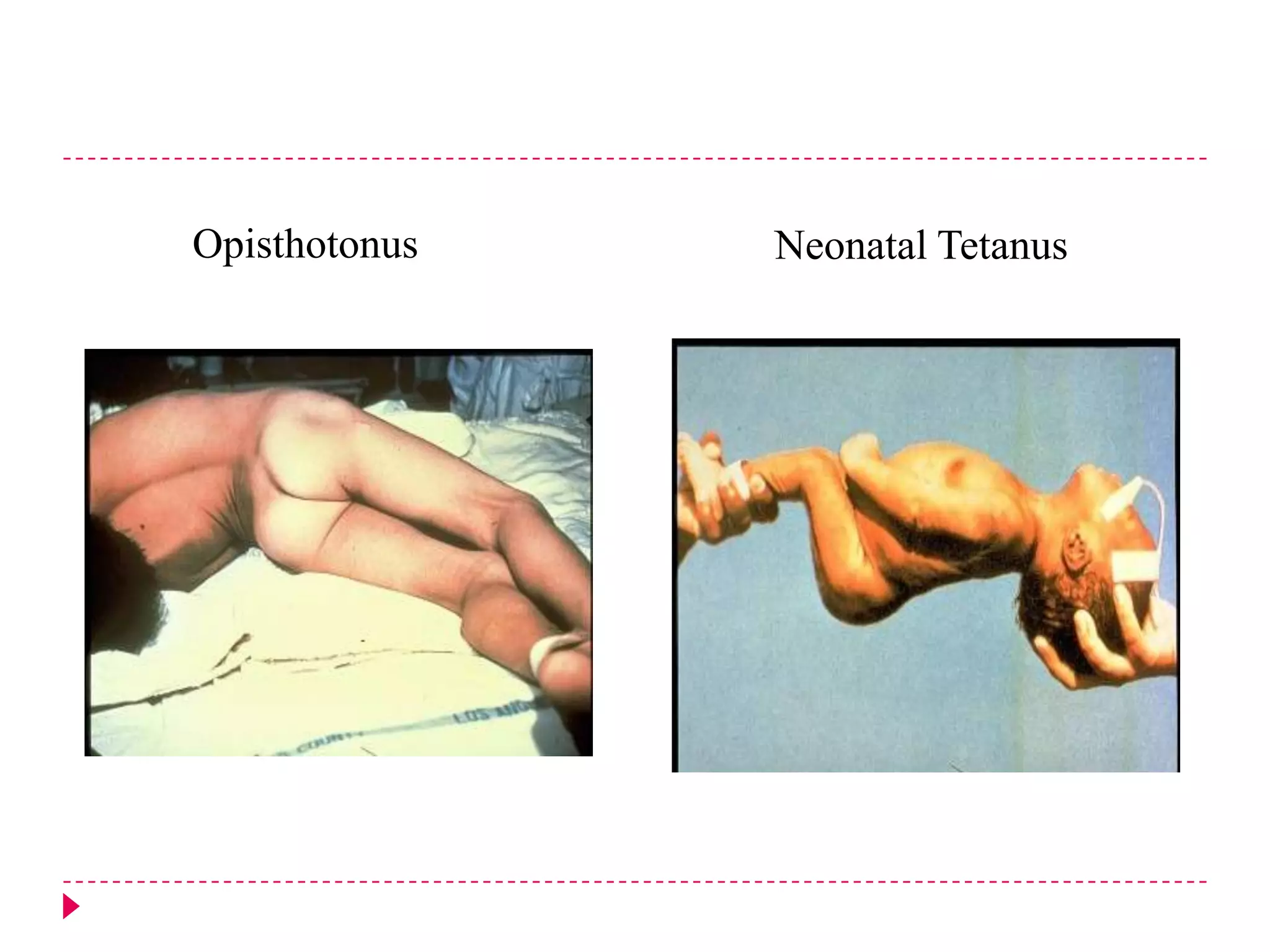

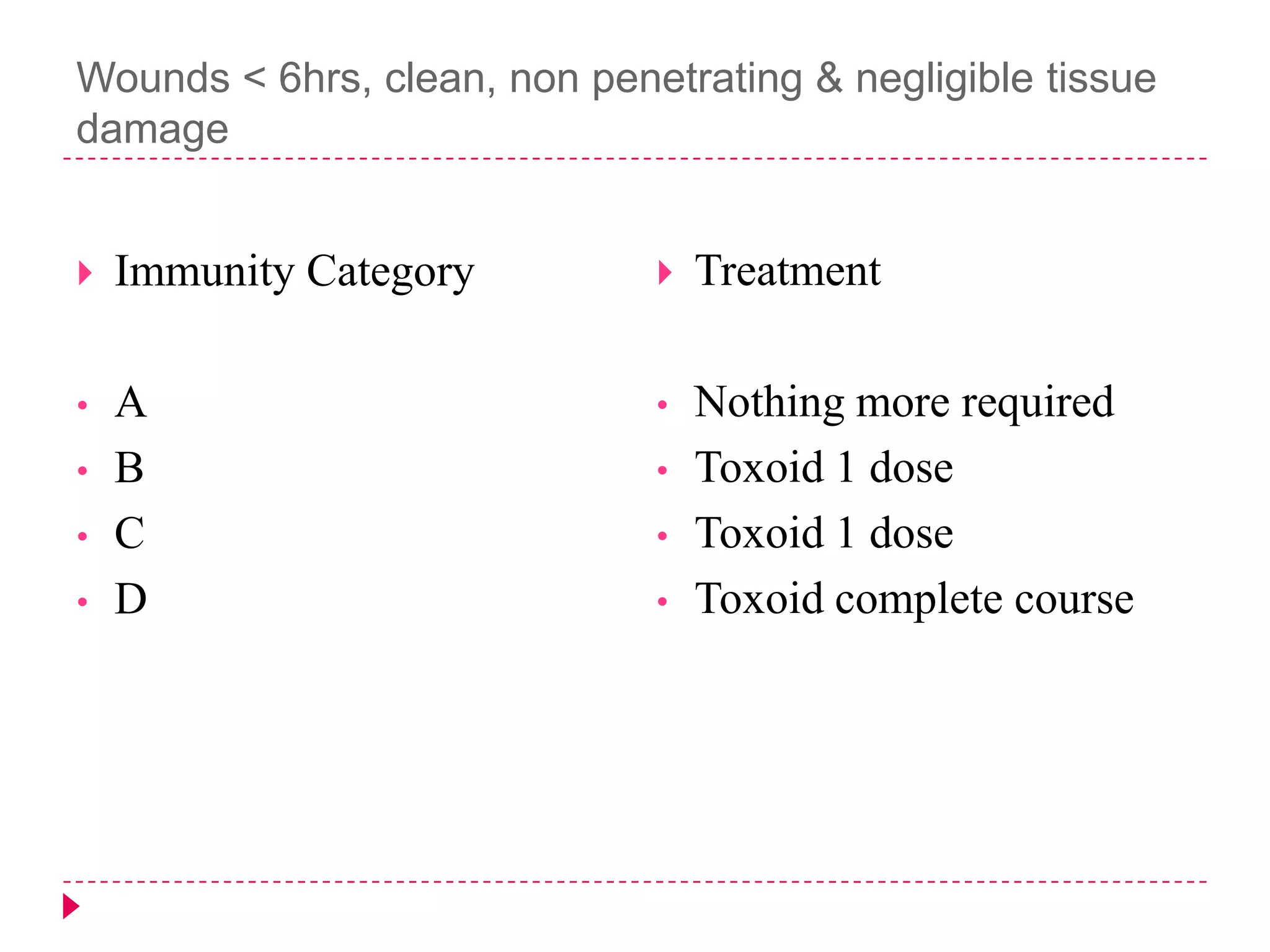
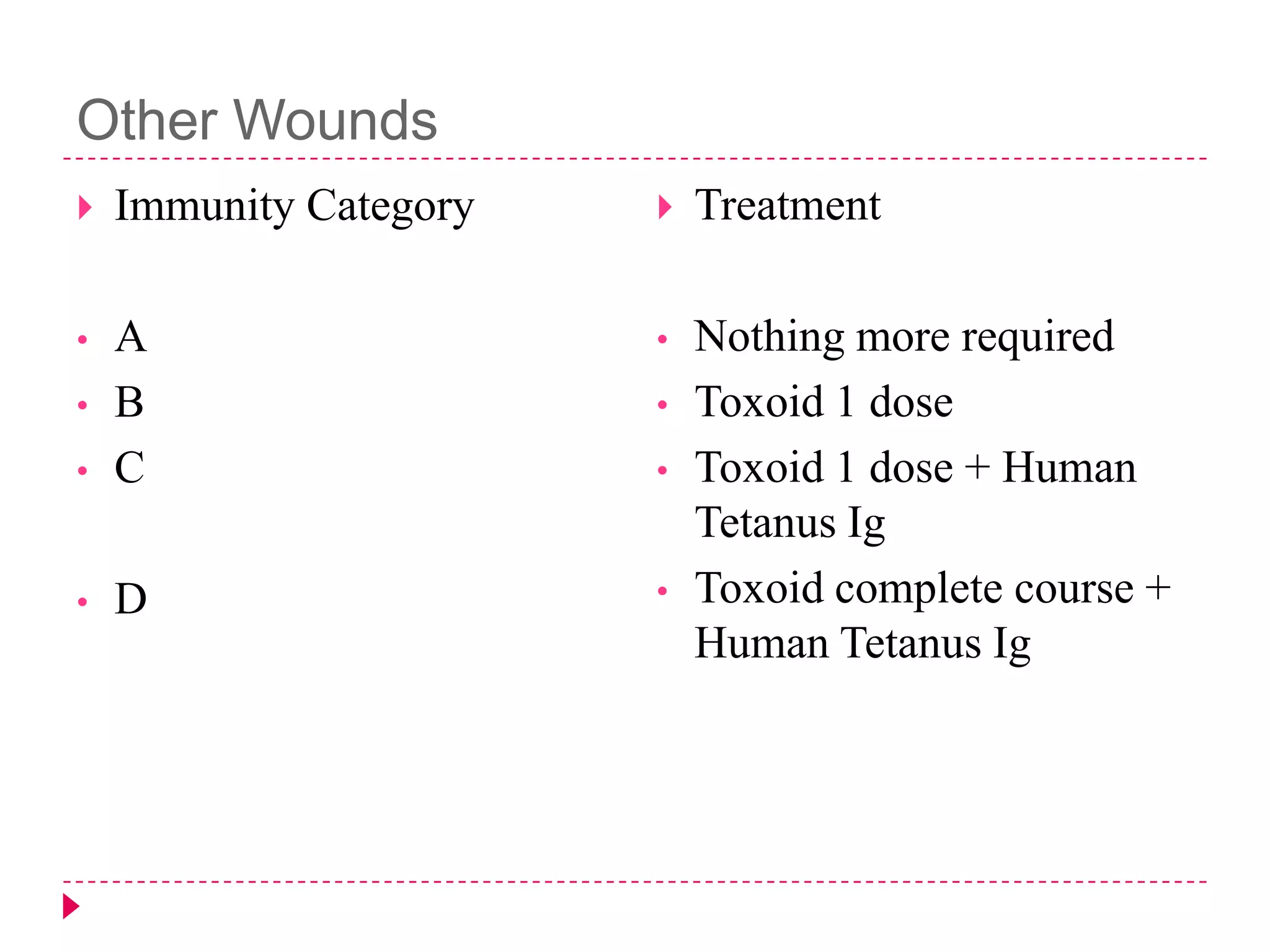

The document details the case of a 60-year-old housewife diagnosed with cephalic tetanus presenting with swallowing difficulties and muscle spasms. It outlines the clinical symptoms, historical context of tetanus, its pathogenesis, and treatment protocols, including the administration of tetanus immunoglobulin and antibiotics. Key points include the importance of timely intervention, prevention through vaccination, and management strategies for autonomic disturbances and muscle spasms.



















































































