
![• Favorable neurologic recovery at hospital discharge
– Hypothermia group: 21/43 pts (49%)
– Normothermia group: 9/34 pts (26%)
– (P = 0.05)
– The odds ratio 5.25 (95% confidence interval [CI], 1.47 to 18.76; P = 0.01),
after adjustment for age and duration of the arrest
Bernard SA, et al. N Engl J Med 2002;346:557-63.](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-14-320.jpg)
![• Multicenter trial
• 275 comatose survivors of a cardiac arrest of
cardiac cause
– VF
– Pulseless VT
• Randomized in 2 groups
– Normothermia
– Hypothermia
• Target temperature, 32 - 34°C
• Cooling duration, 24 hours
• Cooling with the use of cold air
Holtzer M. N Engl J Med 2002;346: 549-56. [Erratum, N Engl J Med 2002;346: 1756.]](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-16-320.jpg)
![Holtzer M. N Engl J Med 2002;346: 549-56. [Erratum, N Engl J Med 2002;346: 1756.]](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-17-320.jpg)
![• Favorable neurologic recovery after 6 months
(good recovery or moderate disability)
– Hypothermia: 75/136 pts (55%)
– Normothermia: 54/137 pts (39%)
• Significant reduction in the rate of death at 6
months
Holtzer M. N Engl J Med 2002;346: 549-56. [Erratum, N Engl J Med 2002;346: 1756.]](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-18-320.jpg)
![P value
0.02
Holtzer M. N Engl J Med 2002;346: 549-56. [Erratum, N Engl J Med 2002;346: 1756.]](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-19-320.jpg)
![The Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl
J Med 2002;346: 549-56. [Erratum, N Engl J Med 2002;346: 1756.]](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-34-320.jpg)
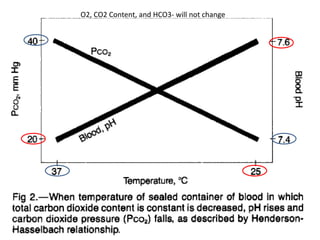
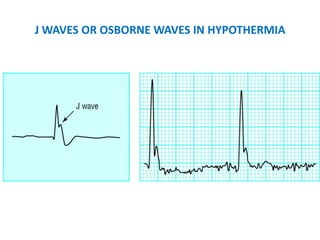
![ABG TEMPERATURE CORRECTION: TO CORRECT OR
NOT TO CORRECT; THAT IS THE QUESTION
• “corrected" : corrected to the pt’s body temperature.
The ABG analyzer readings at the patient's body
temperature
• "non-corrected" : The ABG analyzer readings at 37
• Final recommendation is to assess the acid-base and
oxygenation status by looking at the non-corrected
ABG (at 37 degree) regardless of the patient's actual
temperature
• We need to adjust mechanical ventilation to meet the
patient’s needs
– The goal of achieving normal [PaCO2] and sufficient
oxygenation](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-43-320.jpg)

![HEMODYNAMIC INSTABILITY DURING HYPOTHERMIA
• Rewarming may not be helpful
– Vasodilatation can occur during rewarming
• Fluid replacement
• Inotropics
• Pressors
Holtzer M. N Engl J Med 2002;346: 549-56. [Erratum, N Engl J Med 2002;346: 1756.]](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-48-320.jpg)
![The Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl
J Med 2002;346: 549-56. [Erratum, N Engl J Med 2002;346: 1756.]](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-50-320.jpg)
![The Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl
J Med 2002;346: 549-56. [Erratum, N Engl J Med 2002;346: 1756.]](https://image.slidesharecdn.com/targetedtemperaturemanagementincriticalcare-120116115119-phpapp01/85/Targeted-Temperature-Management-Therapeutic-Hypothermia-in-Critical-Care-Mechanism-of-Benefit-Clinical-Use-and-Recommendations-and-Relevant-Formal-Guidelines-60-320.jpg)

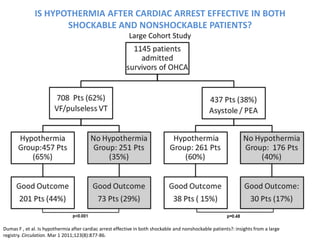
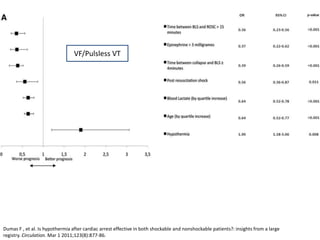
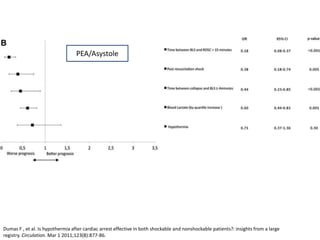
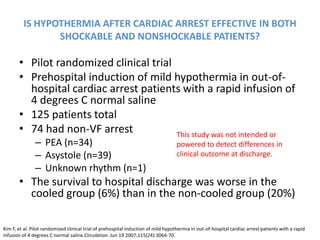
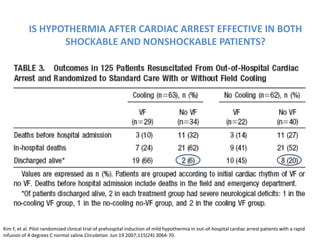
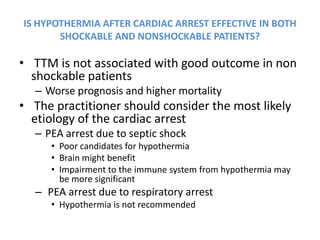
The document discusses targeted temperature management (TTM) in critical care for patients experiencing post-cardiac arrest syndrome, highlighting its benefits in limiting neurological injury and providing clinical guidelines for its use. It includes detailed clinical evidence from trials demonstrating favorable outcomes with TTM, particularly for patients with shockable rhythms, while addressing uncertainties regarding non-shockable cases. Recommendations for TTM initiation, cooling methods, and monitoring practices are also outlined, emphasizing the importance of early intervention and appropriate patient selection.

































![Prehospital induced hypothermia post cardiac arrest jun 2010[1]](https://cdn.slidesharecdn.com/ss_thumbnails/prehospitalinducedhypothermiapost-cardiacarrestjun20101-120131131556-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)