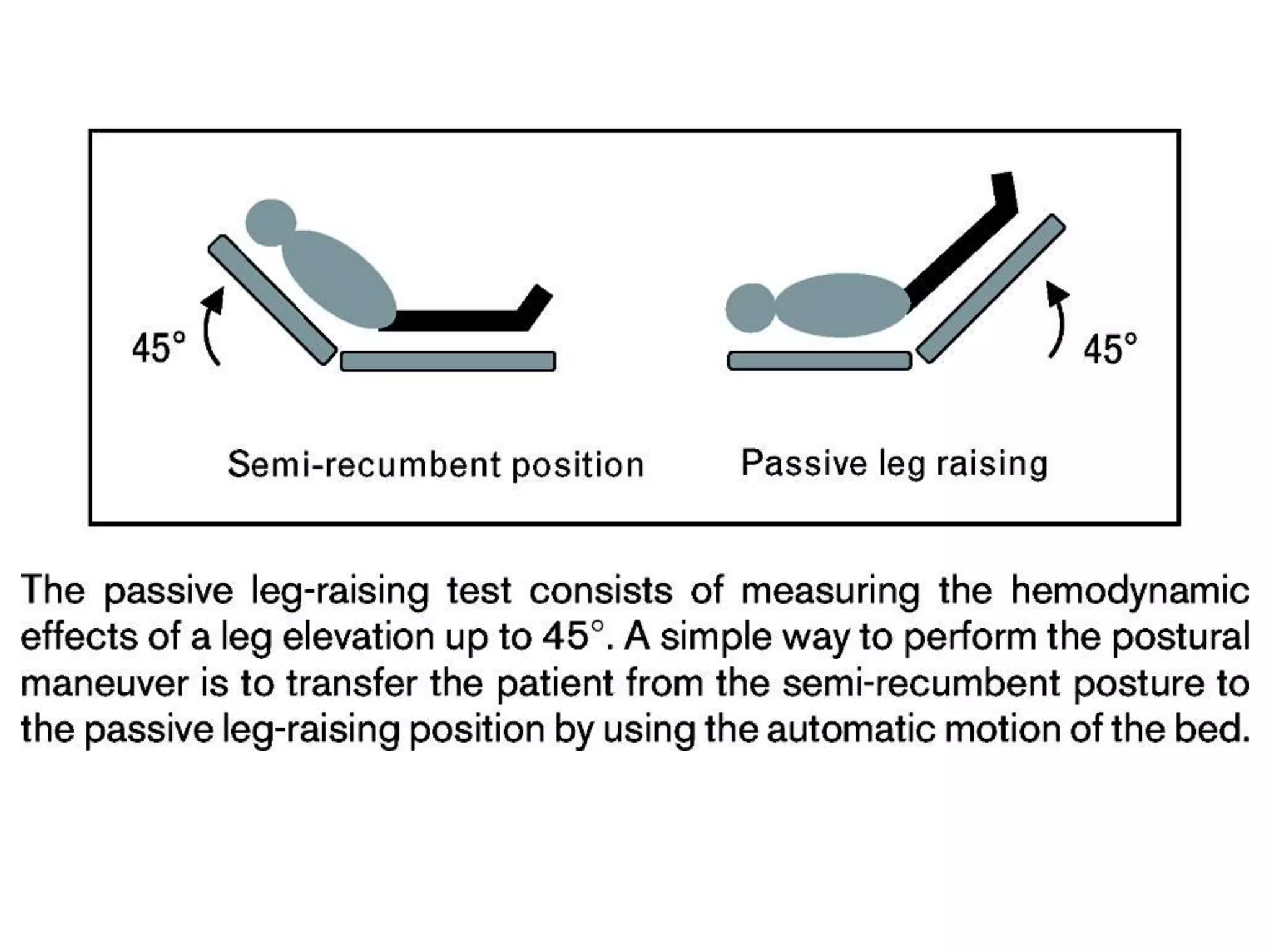
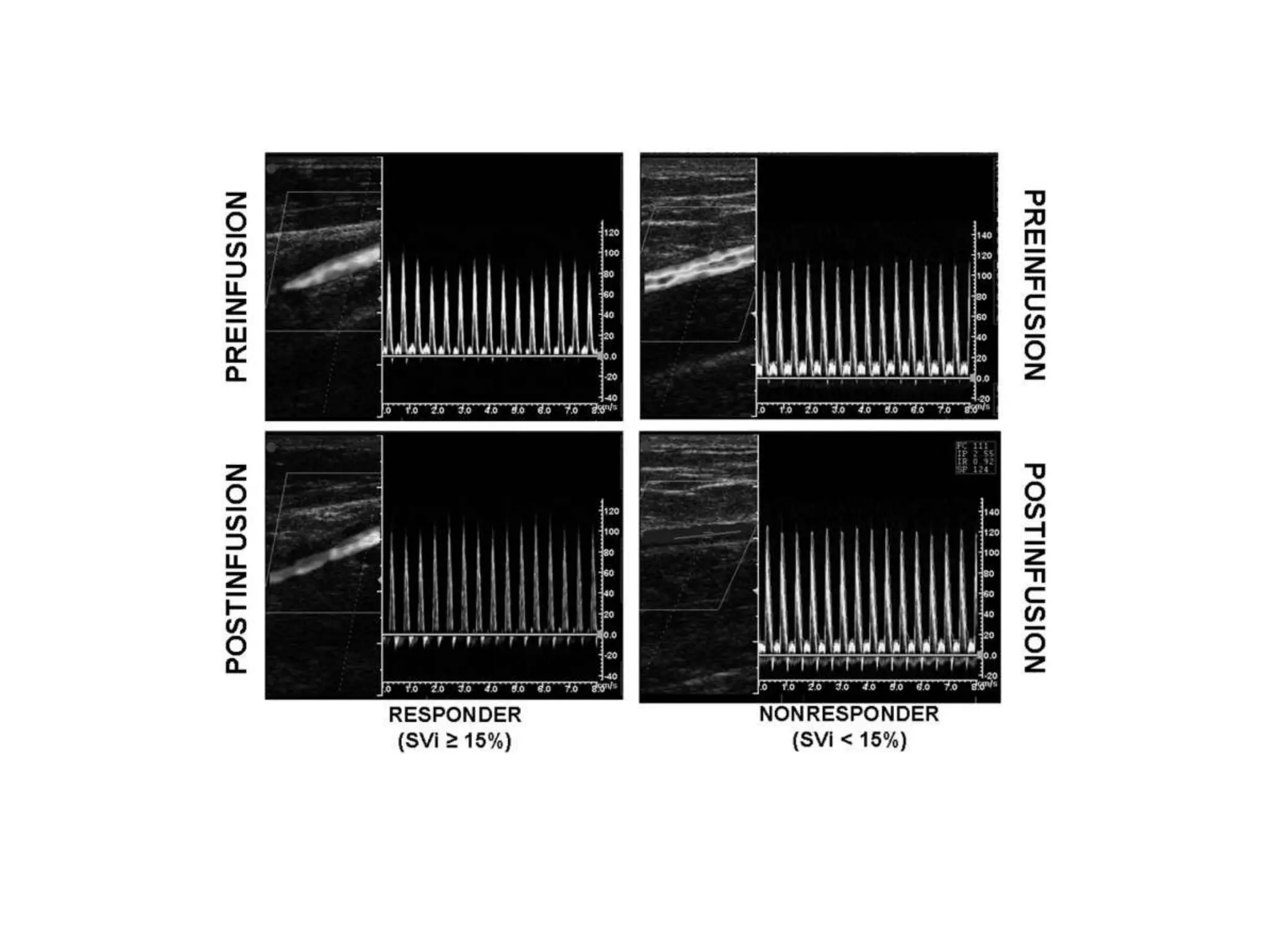
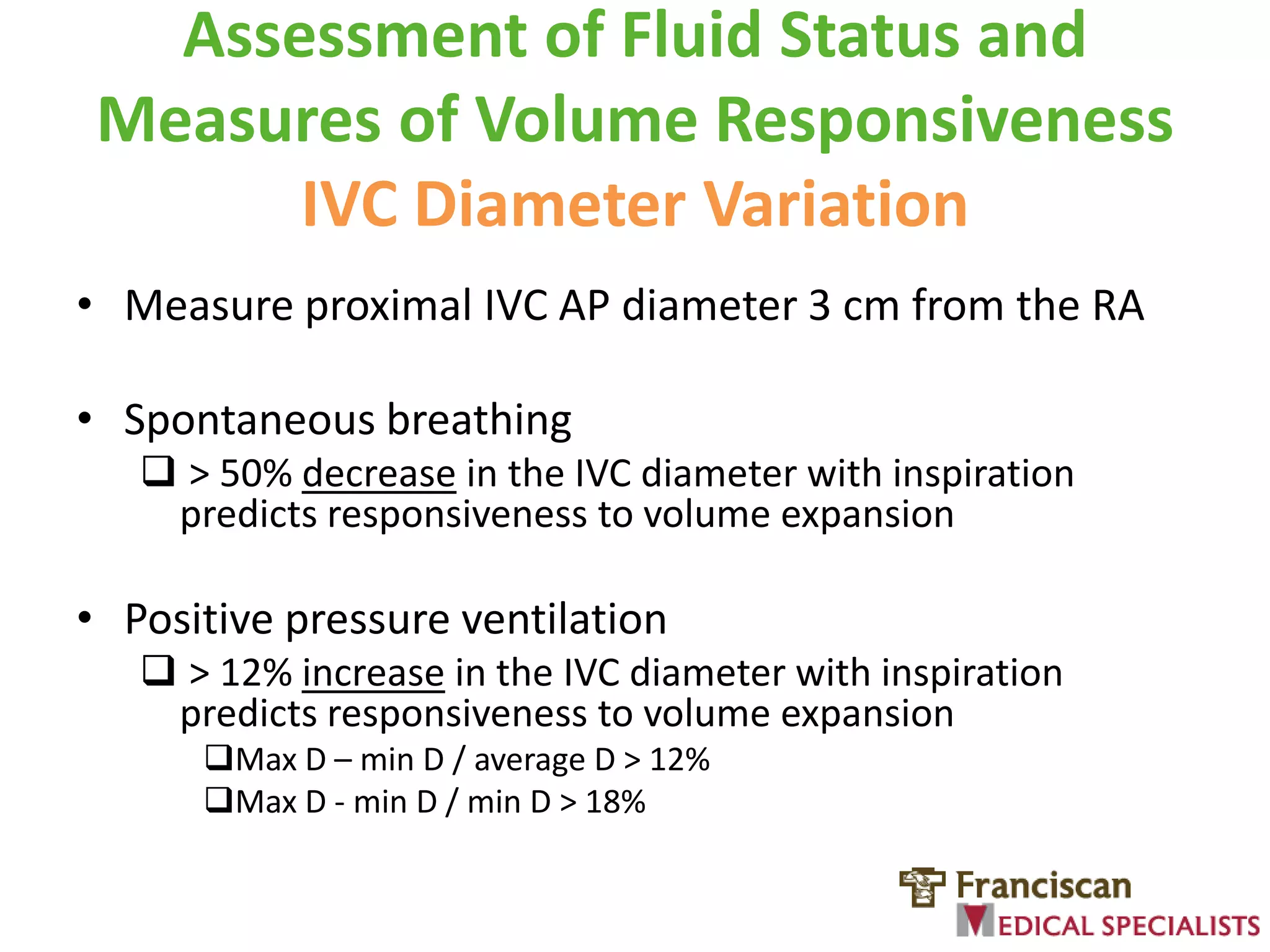
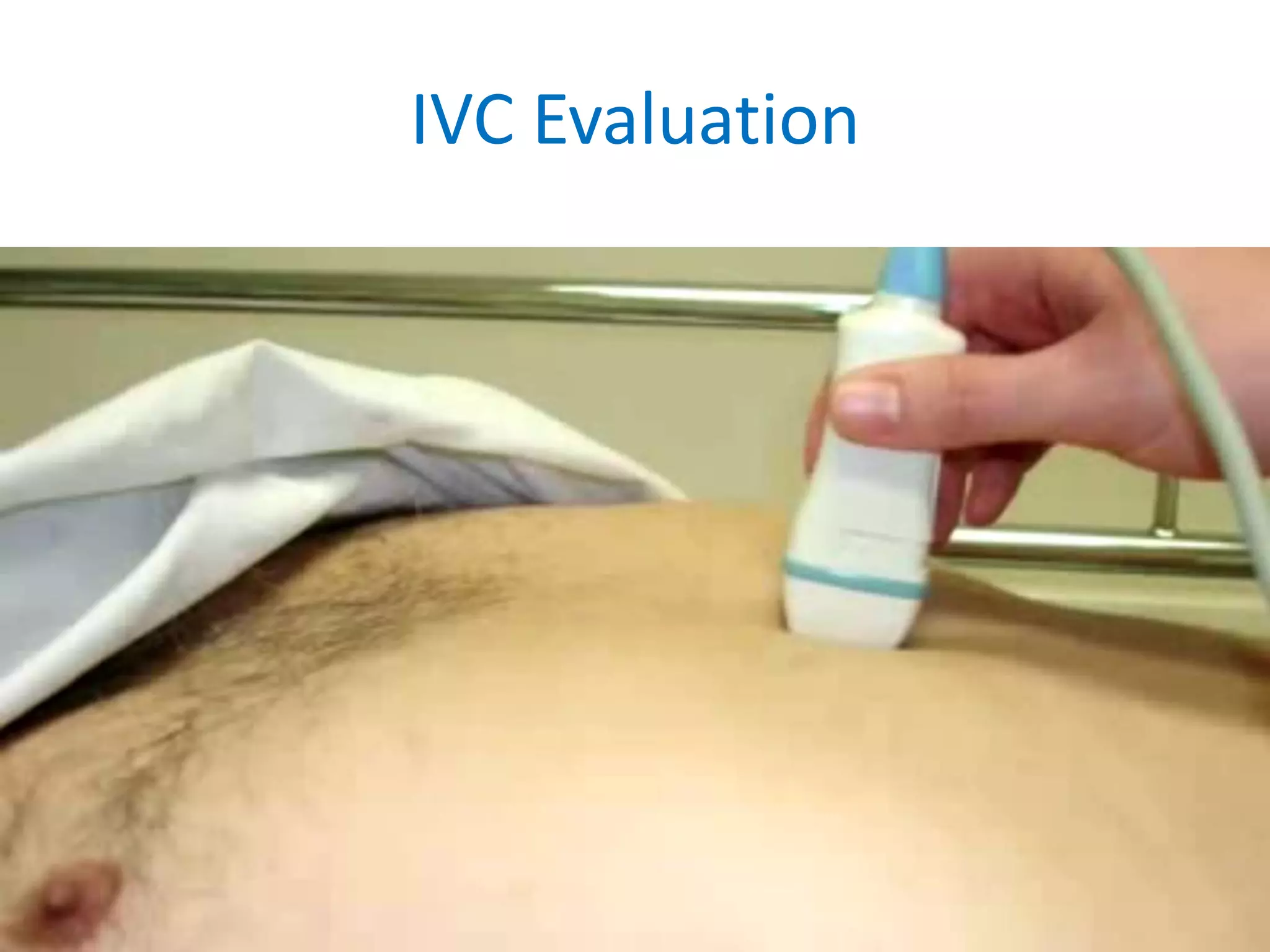
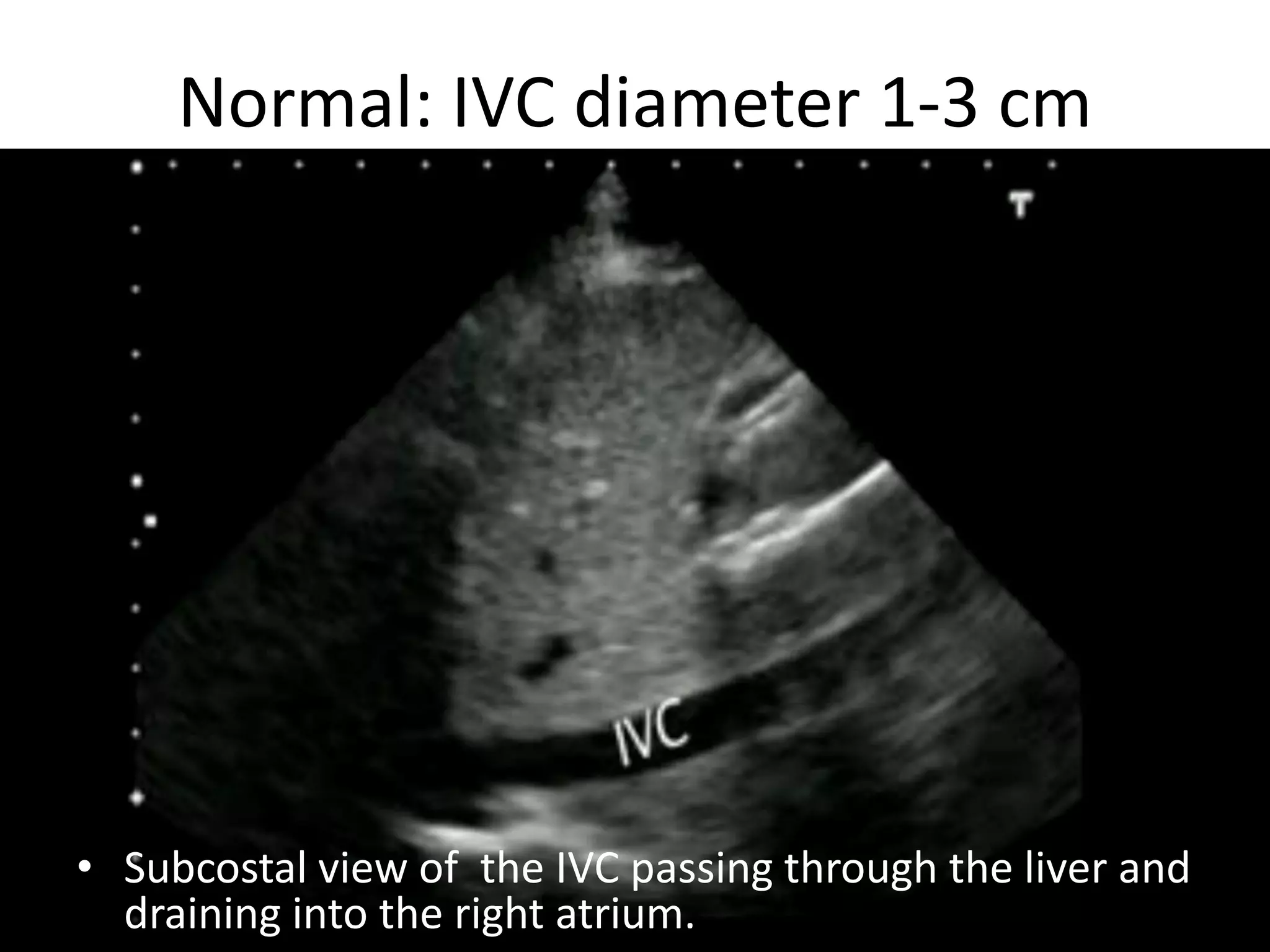
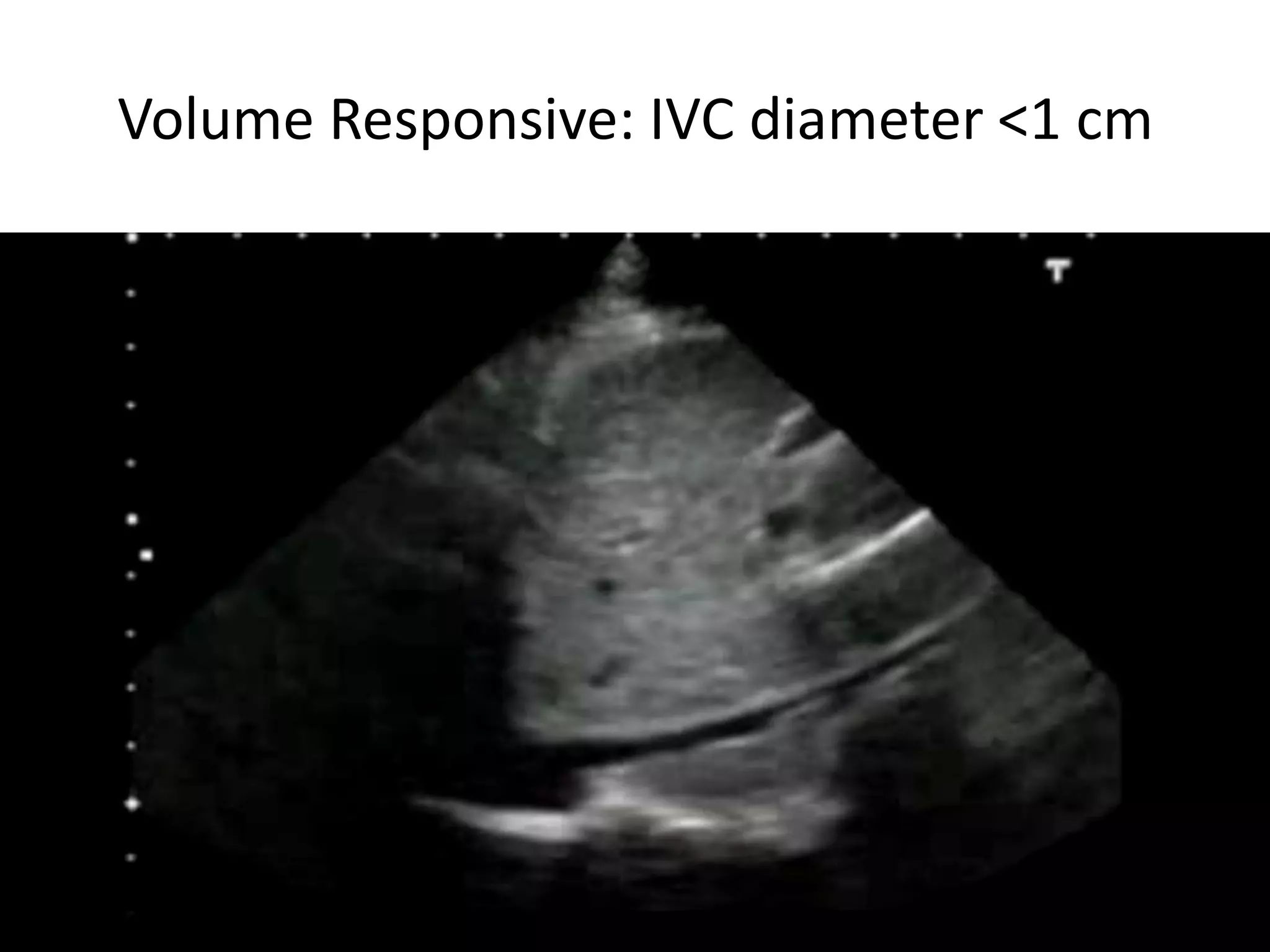
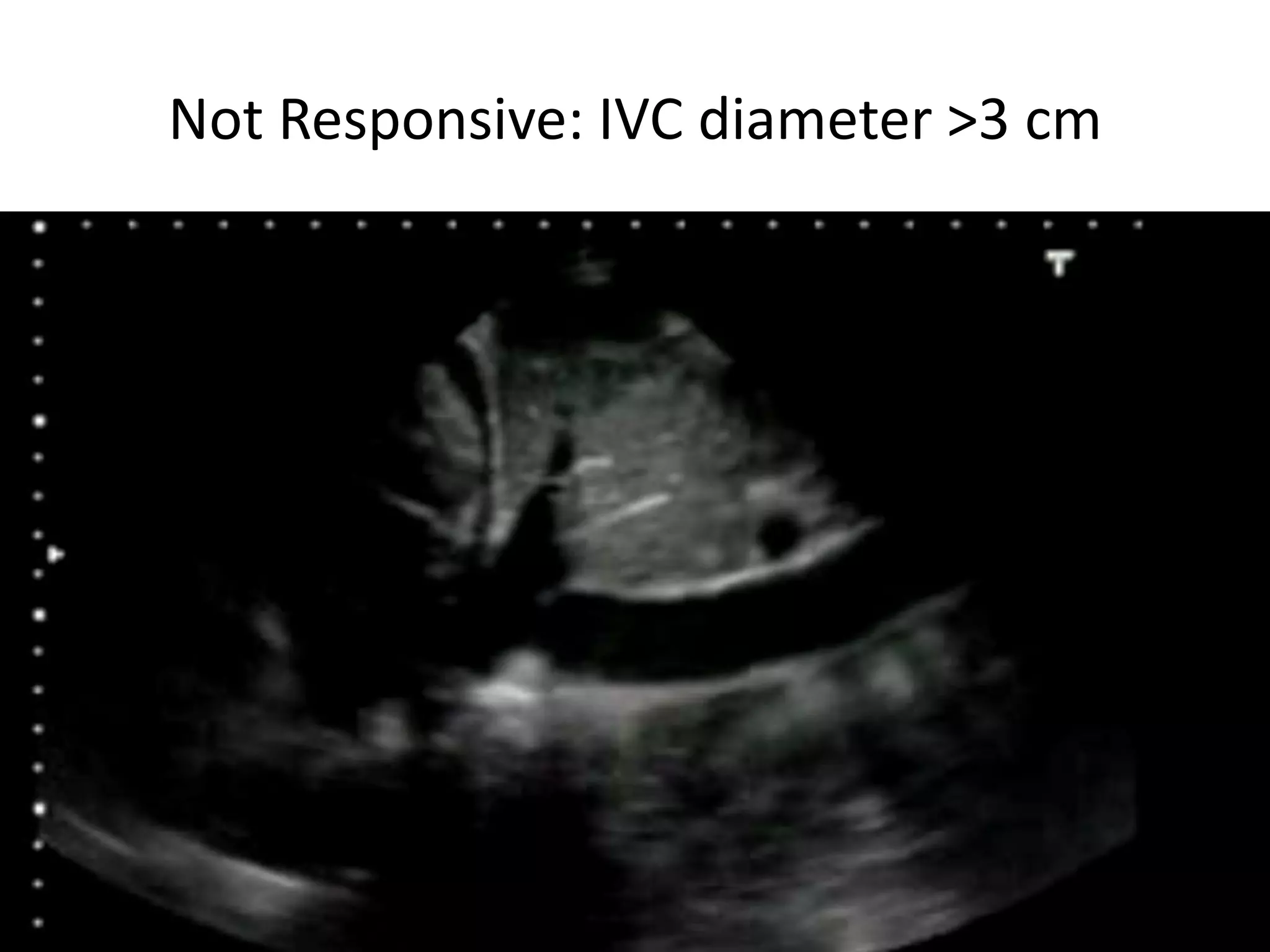
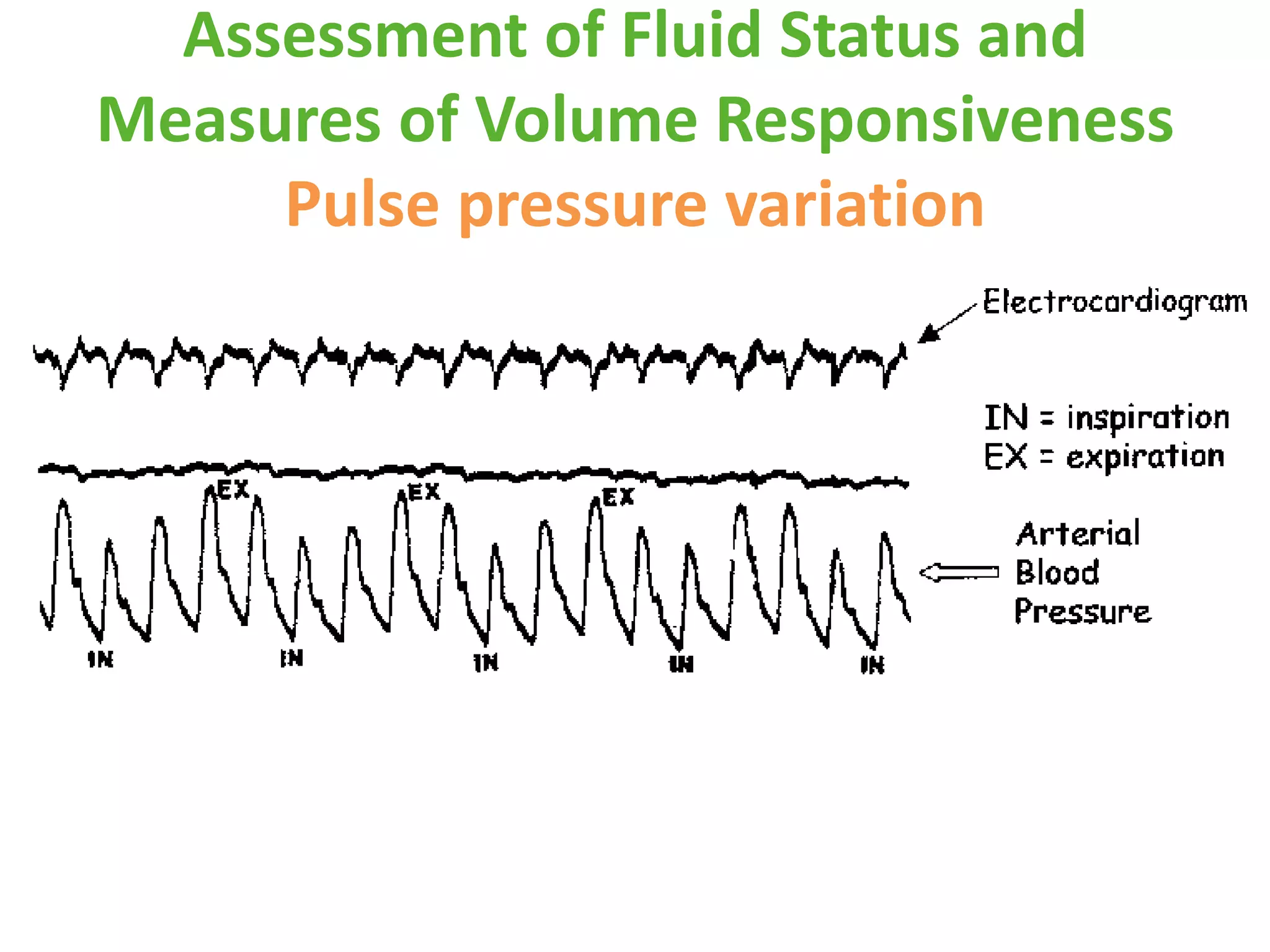

This document discusses hemodynamic monitoring in critically ill patients, focusing on cardiac output, fluid status, and volume responsiveness assessment techniques. It outlines invasive and non-invasive methods for measuring cardiac output, including the Fick principle and pulmonary artery thermodilution, while highlighting their limitations. Additionally, it presents alternative assessments like inferior vena cava diameter variation and passive leg raising tests to evaluate fluid responsiveness.




































































































