Downloaded 580 times


























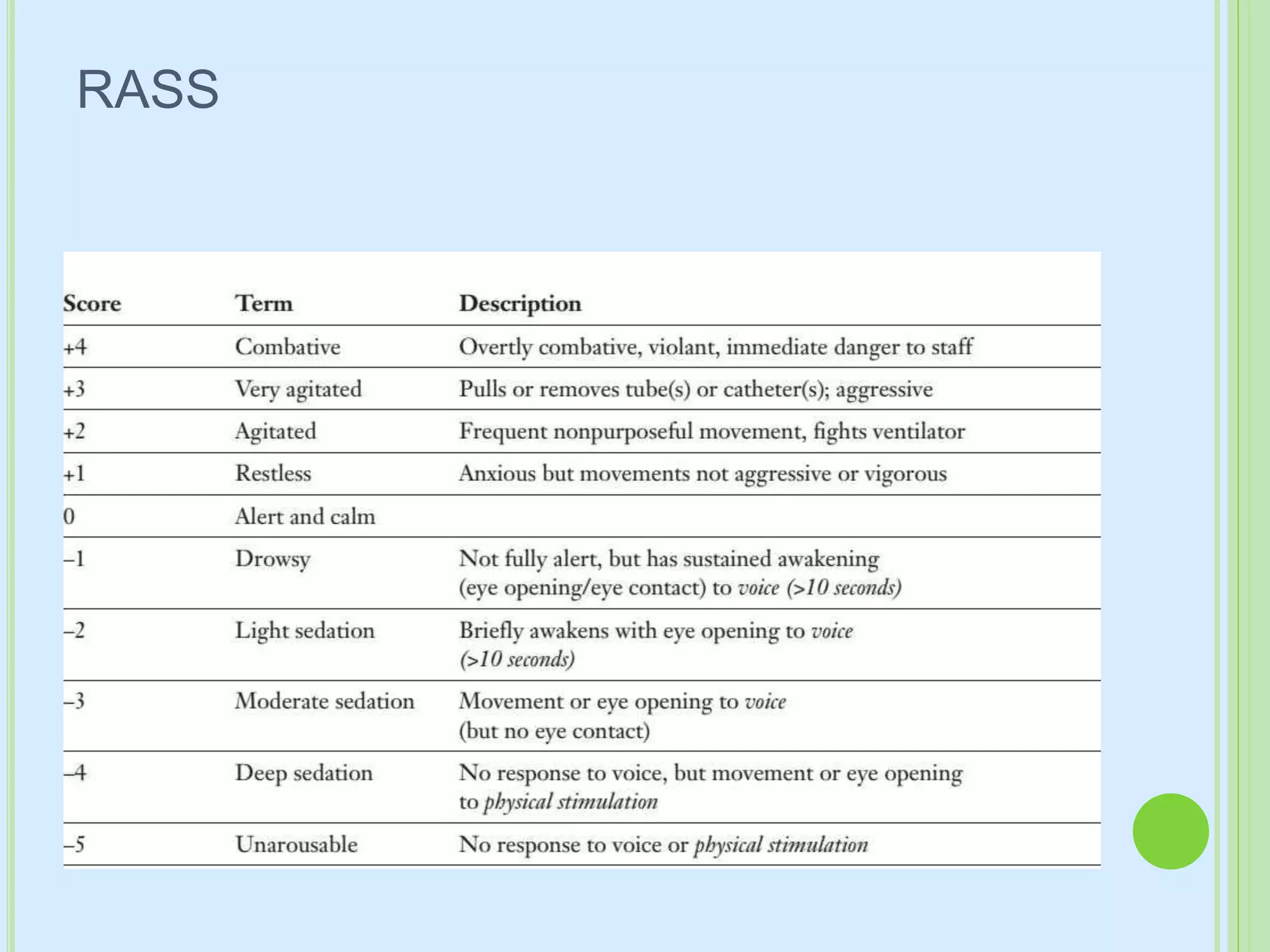
















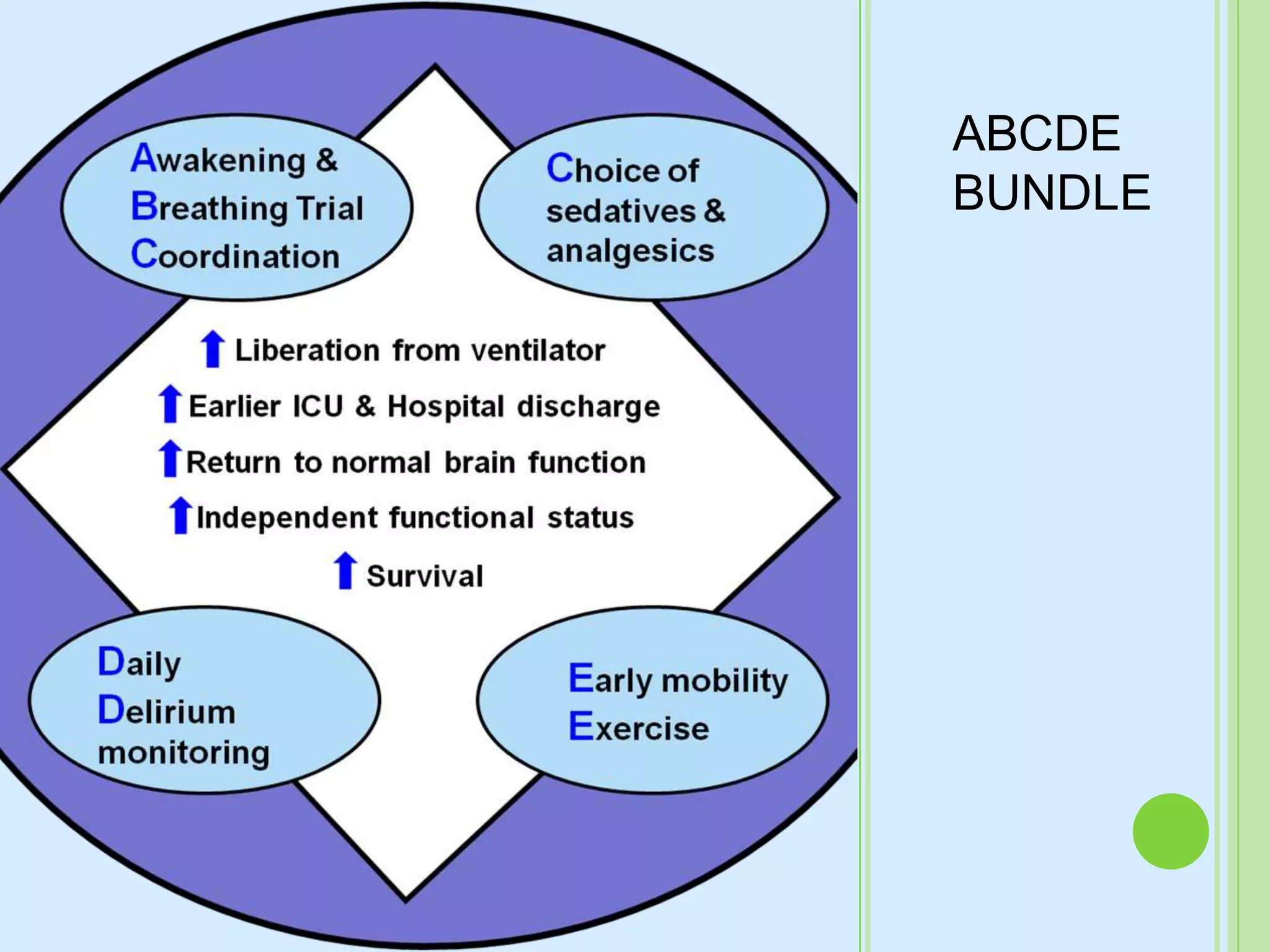





This document provides information on monitoring and managing pain, agitation, and delirium in the ICU. It defines pain, agitation, and delirium and describes scales to monitor them. It discusses various drugs used for analgesia, sedation, and anxiety including opioids, benzodiazepines, propofol, dexmedetomidine, and their dosages, effects, and adverse reactions. It emphasizes the importance of light sedation levels and daily sedation interruption protocols.



































































