
Downloaded 178 times


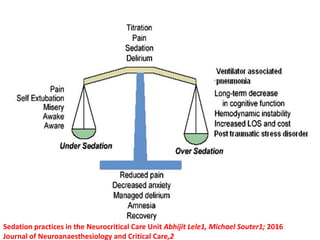
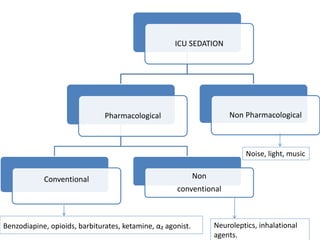



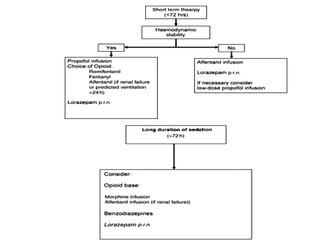
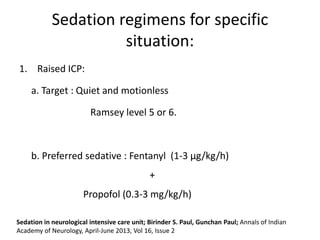
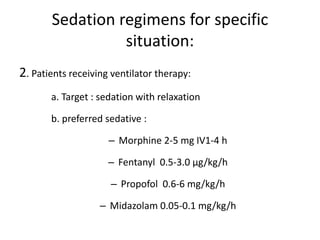

The document discusses the importance and practices of sedation in the neurocritical care unit, highlighting its role in managing intracranial pressure, pain, and agitation. It details various sedation techniques, medications, potential consequences of over- or under-sedation, and assessments to monitor sedation levels. The document emphasizes the need for careful management to optimize patient outcomes while minimizing risks associated with sedation in critically ill neurological patients.























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















