Downloaded 646 times
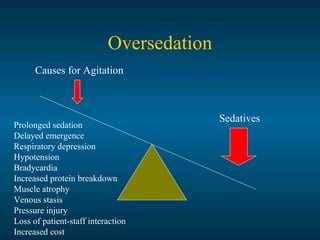
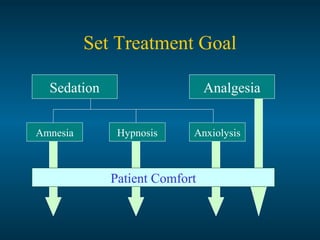
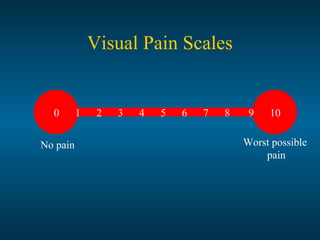
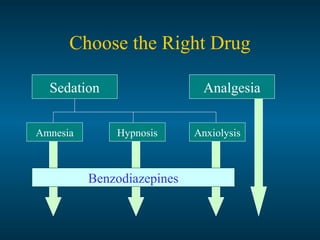
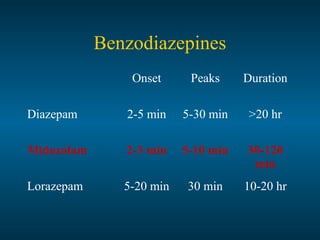
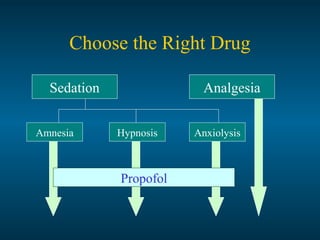
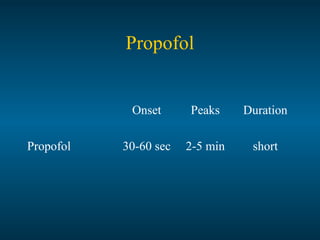
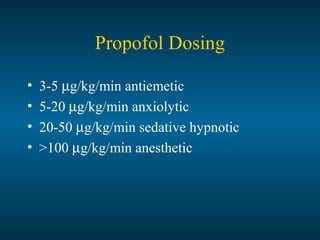
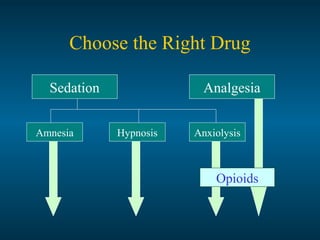
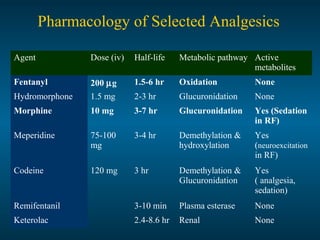
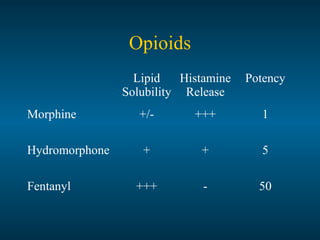
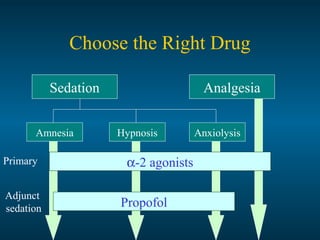
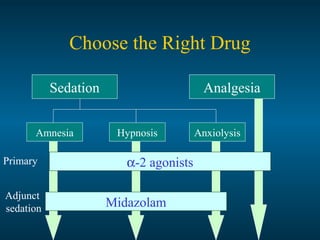
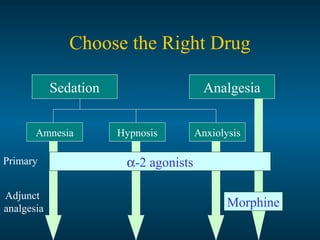
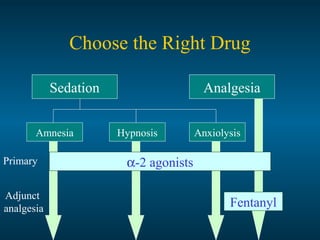

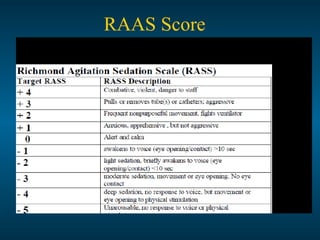




The document discusses sedation, analgesia, and paralysis in the ICU. It describes the goals of sedation as patient comfort while allowing interaction. The challenges include assessing sedation and altered drug pharmacology. An ideal sedation agent would have rapid onset and offset and lack respiratory depression. Monitoring scales like the Richmond Agitation Scale are used to standardize treatment. Dexmedetomidine, propofol, opioids and paralytics may be used. The optimal sedation approach balances adequate treatment while avoiding oversedation risks.















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)







