Downloaded 262 times


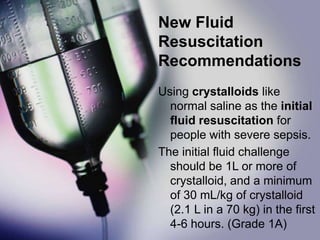











The document summarizes updated guidelines from the 41th Society of Critical Care Medicine Meeting for treating sepsis. Key changes include recommending crystalloids like saline for initial fluid resuscitation; using norepinephrine as the first choice vasopressor; considering corticosteroids for refractory shock; using higher PEEP and recruitment maneuvers for ARDS; and considering procalcitonin to determine if antibiotics can be stopped. The Surviving Sepsis guidelines were previously criticized for being funded primarily by Eli Lilly without disclosure.