Downloaded 183 times

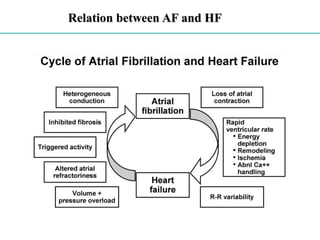
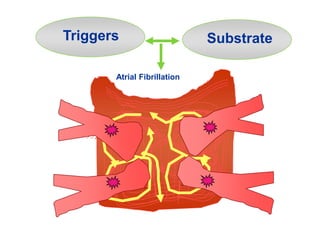



Tachycardia induced cardiomyopathy is a type of dilated cardiomyopathy caused by chronic or frequent tachycardia that leads to impaired left ventricular function. This impairment is partially or fully reversible by controlling the heart rate. The document discusses the criteria, types, pathophysiology, diagnosis, and treatment of tachycardia induced cardiomyopathy. Treatment focuses on heart rate control through medications, ablation, or devices, which can improve ejection fraction and heart failure symptoms over time.






















































































