Downloaded 153 times

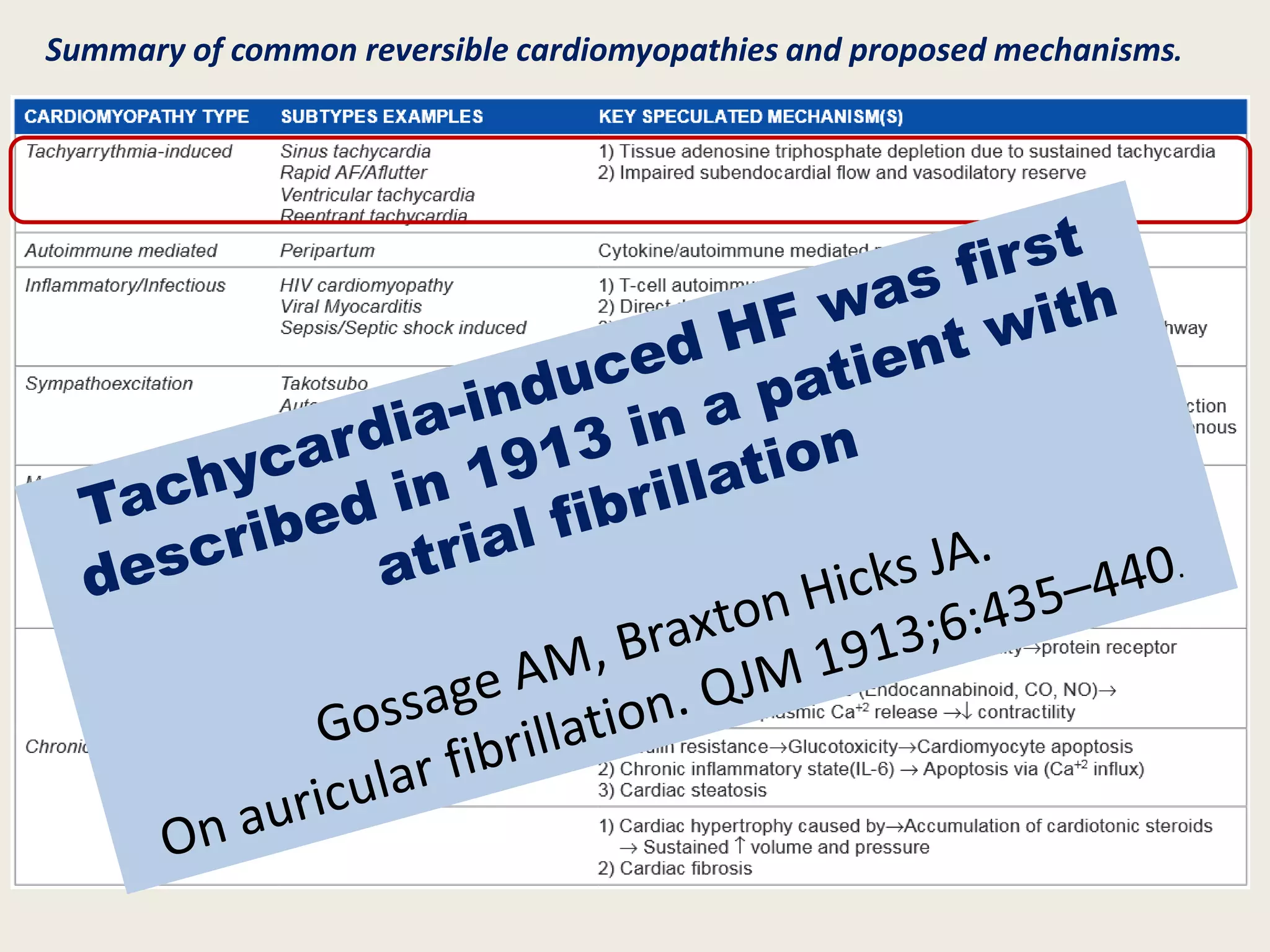

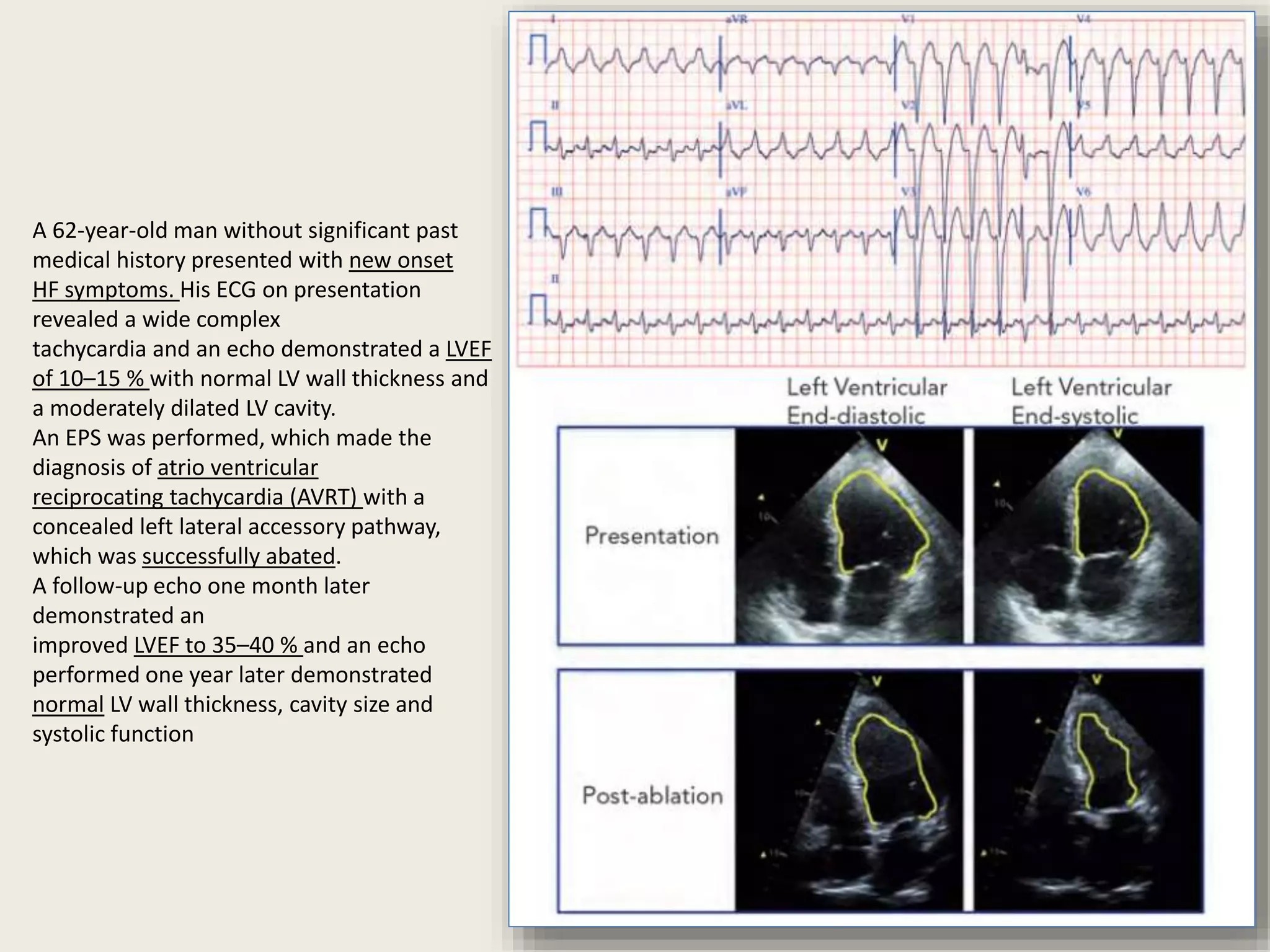

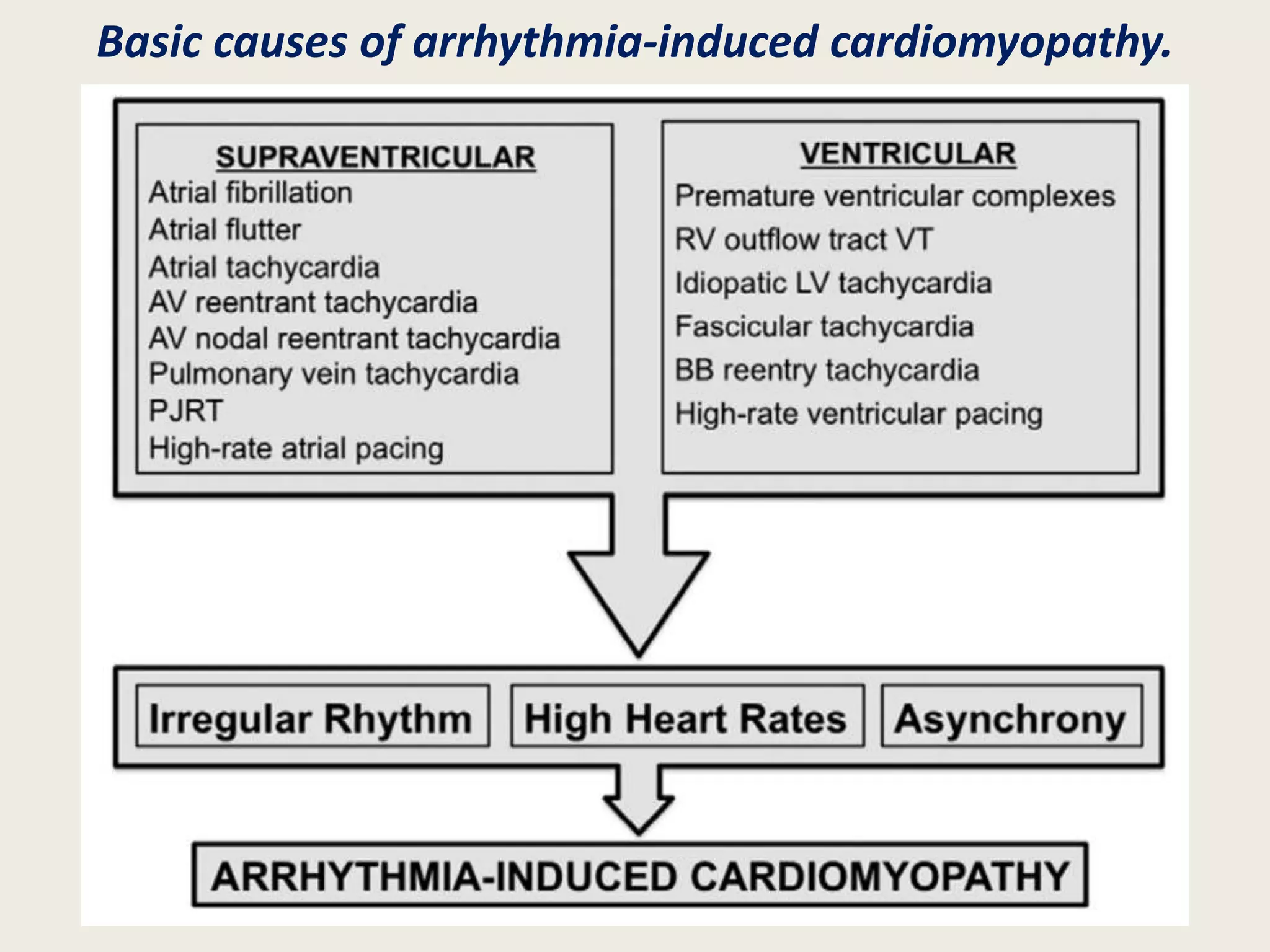

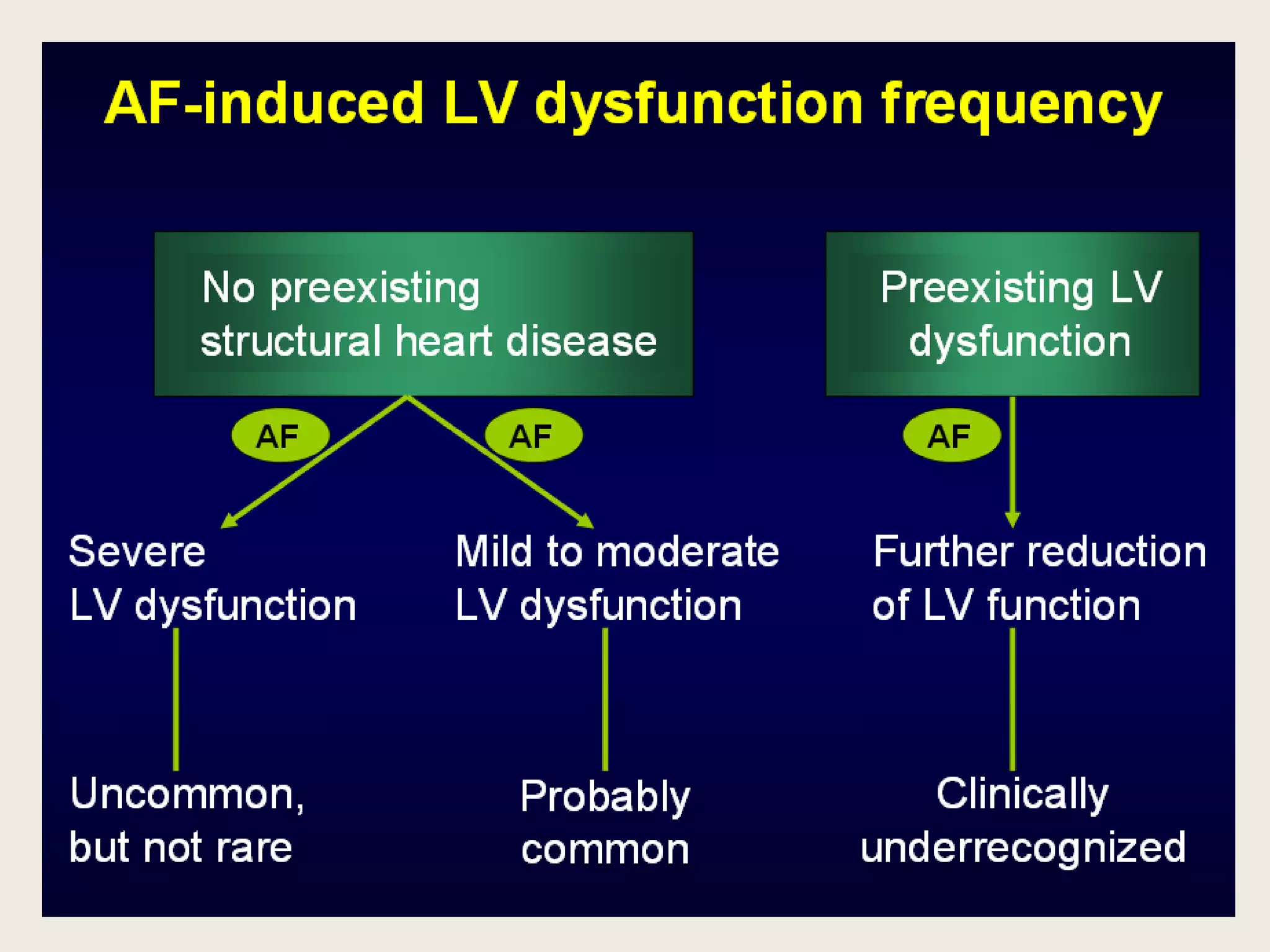

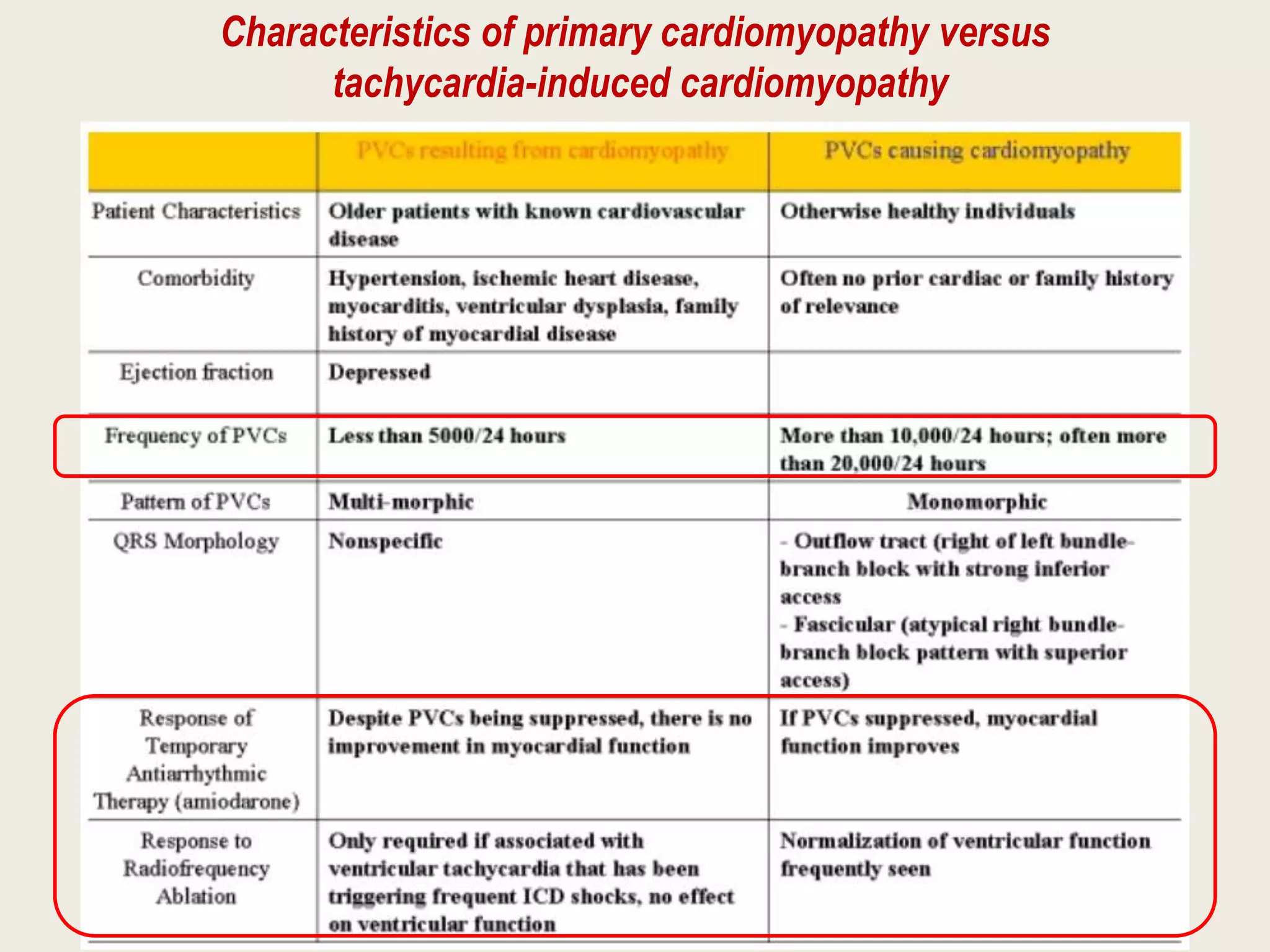

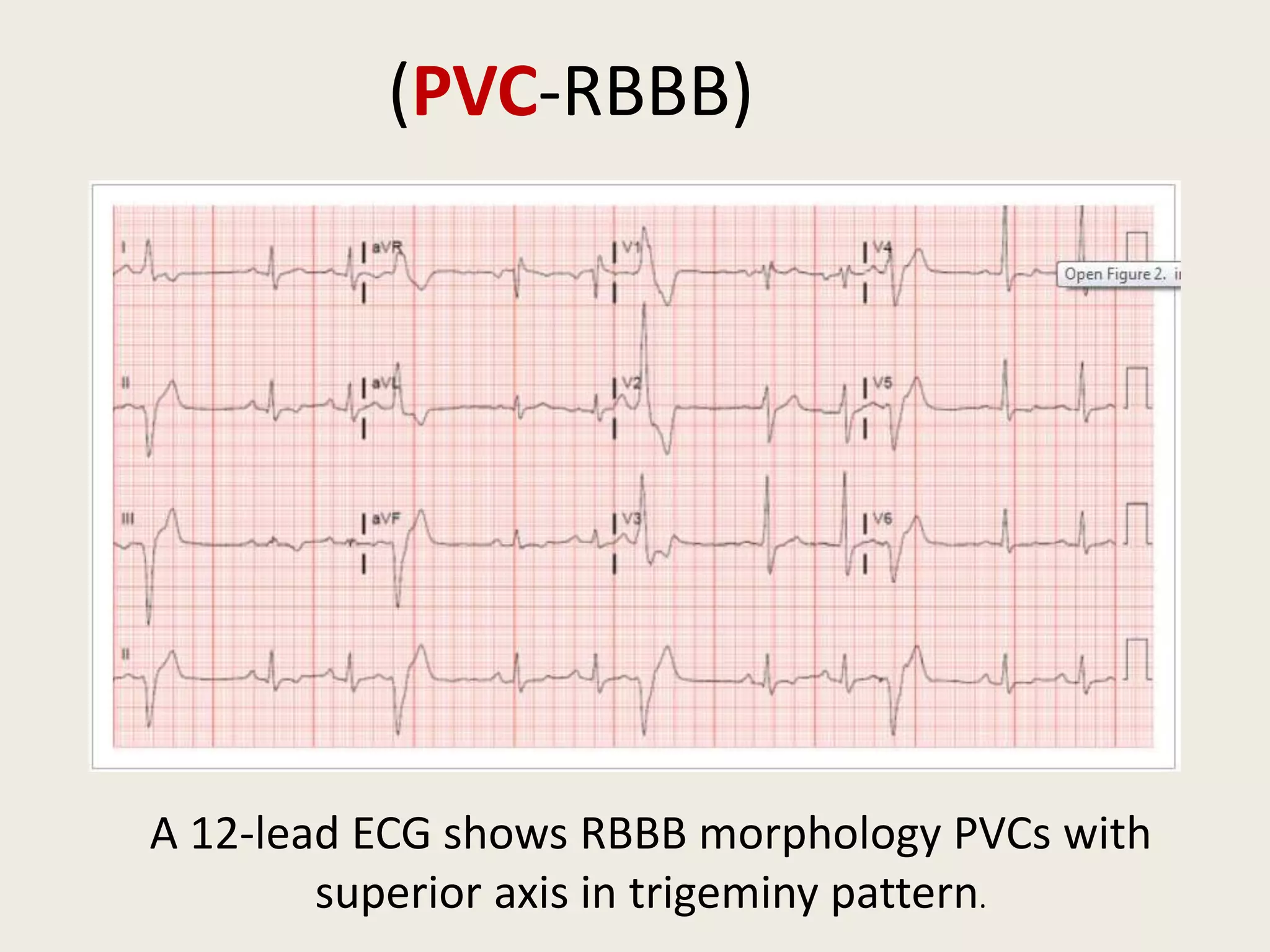








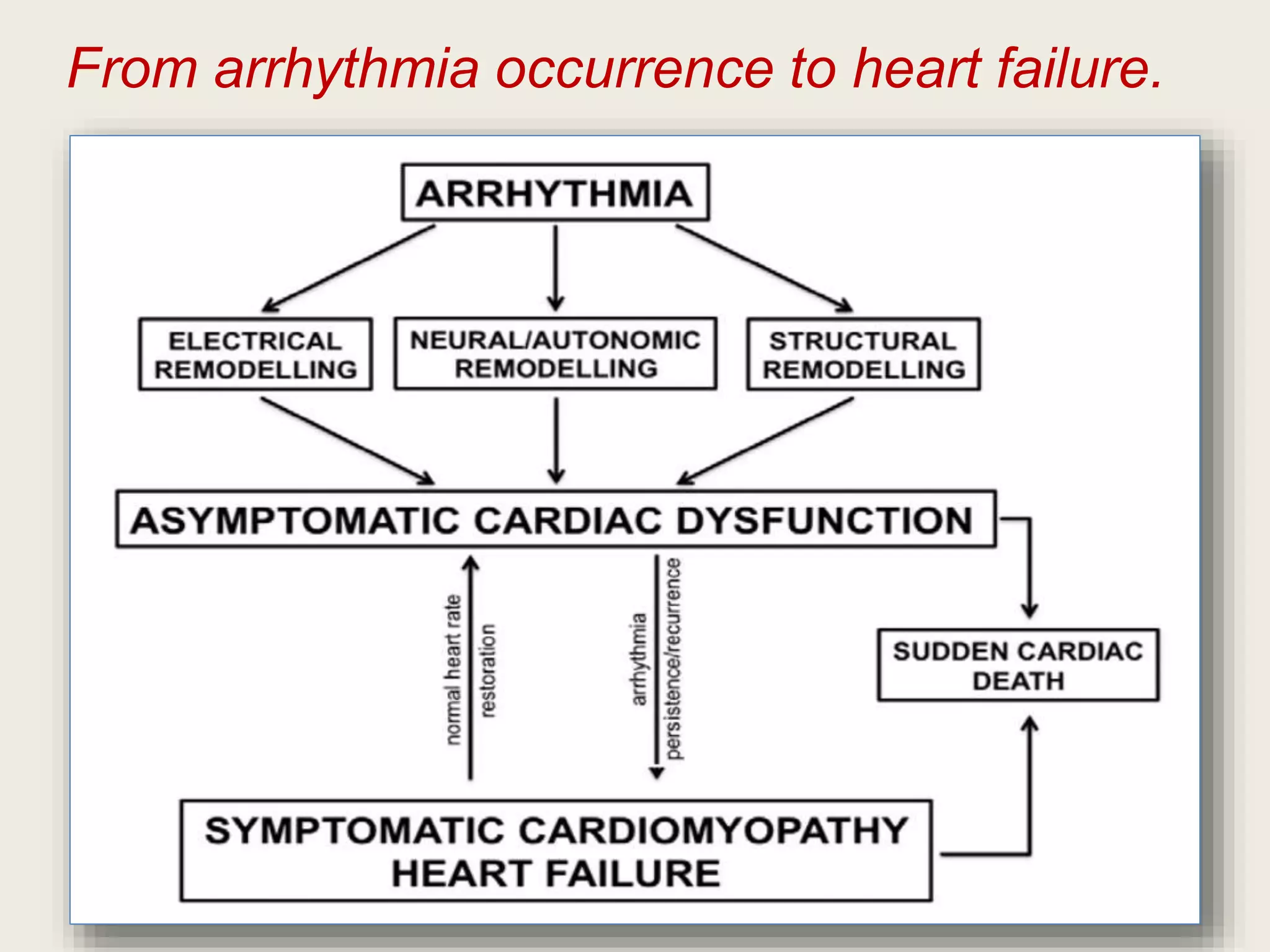



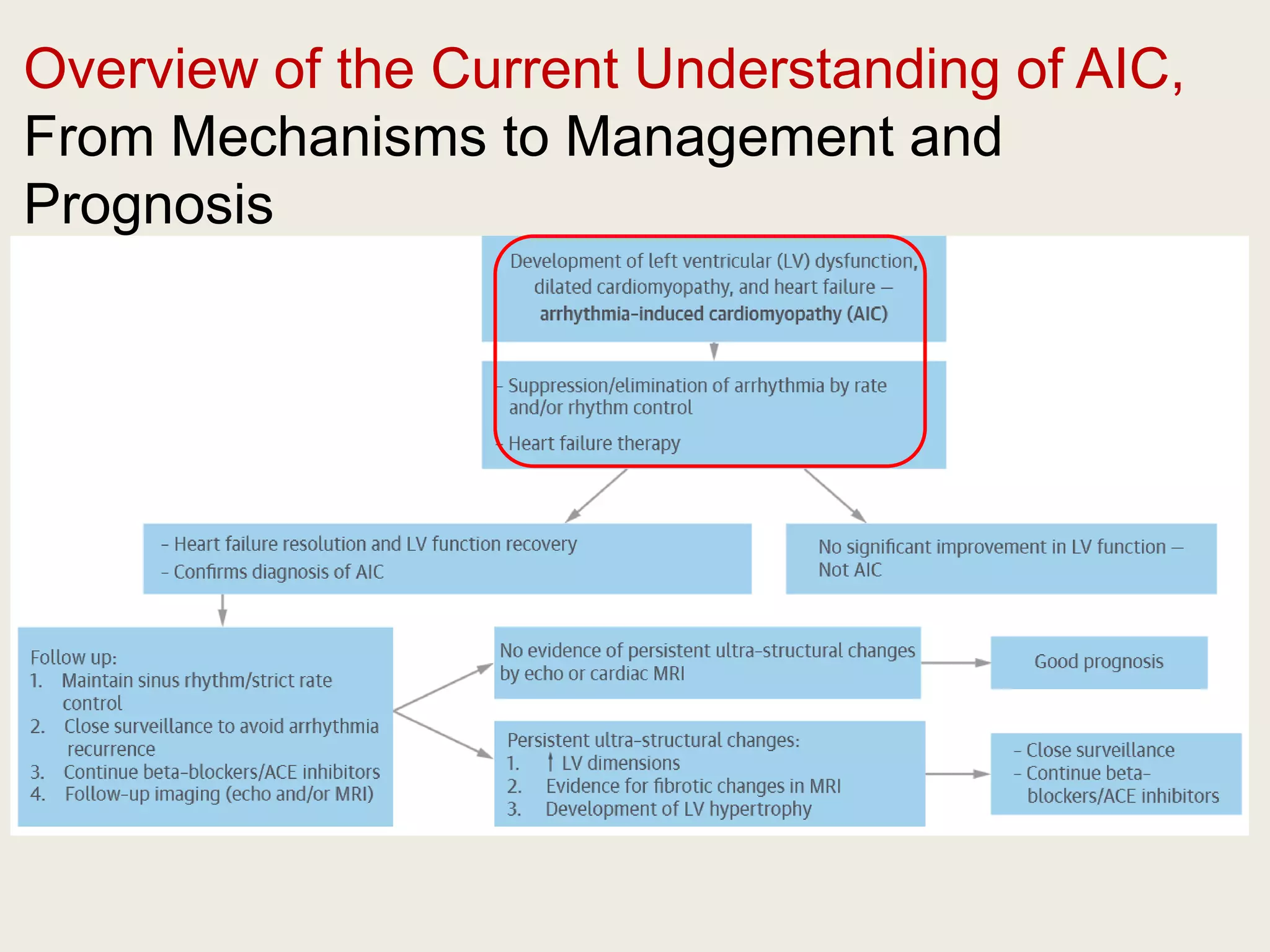


The document discusses reversible cardiomyopathies, particularly focusing on arrhythmia-induced cardiomyopathy (AIC), which can lead to severe left ventricular dysfunction and heart failure due to tachyarrhythmias. It emphasizes the importance of addressing the arrhythmia, as improvement in heart function may occur once it is controlled, and outlines management strategies such as catheter ablation and antiarrhythmic therapy. The text also highlights challenges in identifying the causative factors of AIC and the need for careful monitoring due to risks of recurrence and sudden cardiac events.





























































































