Downloaded 21 times
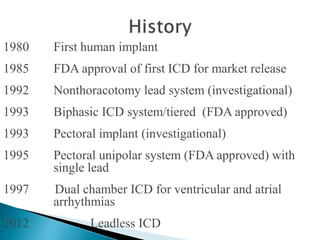

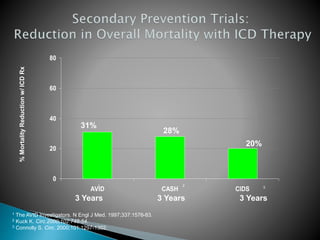
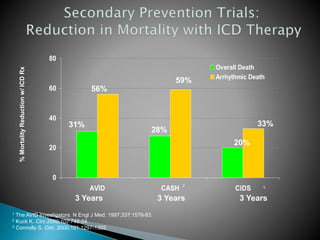
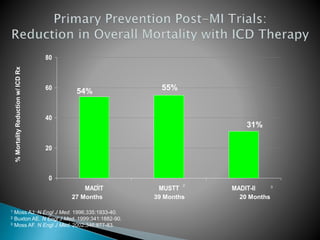
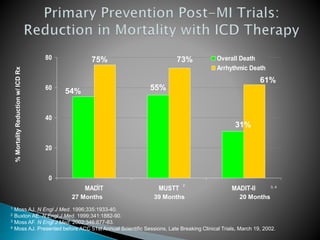
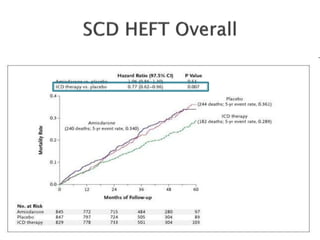
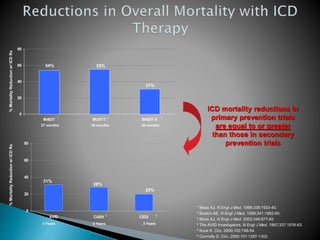
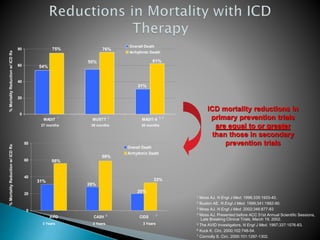


The document discusses the history and development of implantable cardioverter defibrillators (ICDs) from their introduction in 1980 through dual chamber ICDs in 1997 and leadless ICDs in 2012. It then summarizes several major clinical trials that demonstrated the mortality benefits of ICD therapy in both primary and secondary prevention of sudden cardiac death. These trials showed reductions in overall mortality ranging from 20-55% and reductions in arrhythmic mortality ranging from 28-75% with ICD therapy.

























![Ambulatory blood pressure monitoring [abpm]](https://cdn.slidesharecdn.com/ss_thumbnails/ambulatorybloodpressuremonitoringabpm-140314094820-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























































