Downloaded 50 times
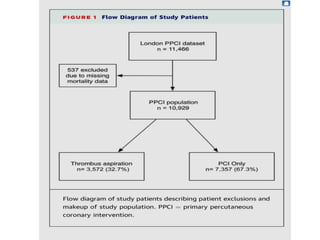
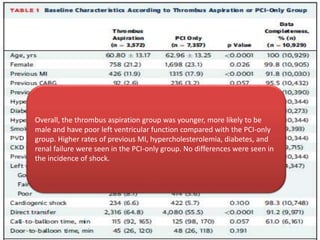
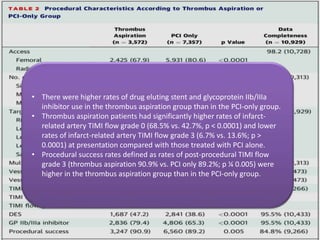
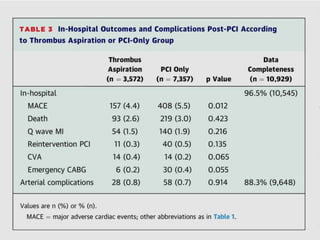
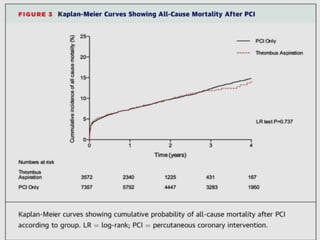
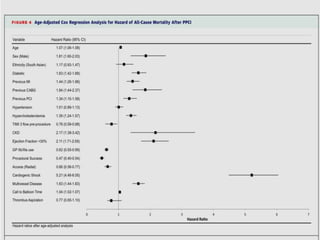
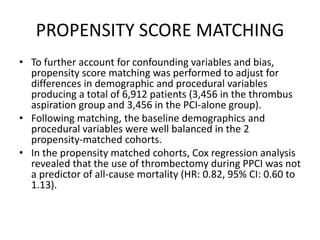

Manual thrombus aspiration during primary percutaneous coronary intervention (PPCI) for ST-segment elevation myocardial infarction (STEMI) was not associated with reduced long-term mortality according to a study of 10,929 patients. While thrombus aspiration was linked to higher procedural success rates and lower in-hospital complications, long-term survival was similar between patients who received thrombus aspiration and those who underwent PPCI only. After adjusting for differences in patient characteristics and procedures using propensity score matching, thrombus aspiration during PPCI was still not found to reduce mortality risk.








































![Ambulatory blood pressure monitoring [abpm]](https://cdn.slidesharecdn.com/ss_thumbnails/ambulatorybloodpressuremonitoringabpm-140314094820-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)














































