Downloaded 304 times
![MICROSCOPY
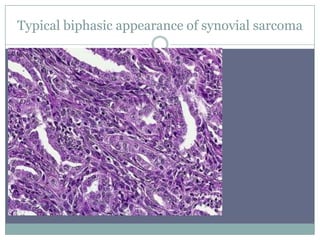
Biphasic tumor composed of sharply segregated
epithelial and sarcomatous components
The epithelial areas usually appear in the form of
gland-like spaces lined by cuboidal or columnar
cells, but can also present as solid nests of large pale
cells. It is exceptional for this component to exhibit
squamous features.[1537]](https://image.slidesharecdn.com/sncar-130829091317-phpapp01/85/SYNOVIAL-CELL-SARCOMA-DR-NARMADA-11-320.jpg)
![SPECIAL STAIN
Special stains: Histochemistry- Secretions within
the epithelial cell and pseudoglandular spaces
are PAS positive and diastase resistant, alcian
blue and mucicarmine positive.
The stromal mucin secreted by the spindle cells
are alcian blue positive but PAS negative.
Reticulin stain demonstrate the biphasic pattern
of the tumor. Nests of plump rounded cells are
highlighted by the reticulin stain.]](https://image.slidesharecdn.com/sncar-130829091317-phpapp01/85/SYNOVIAL-CELL-SARCOMA-DR-NARMADA-22-320.jpg)
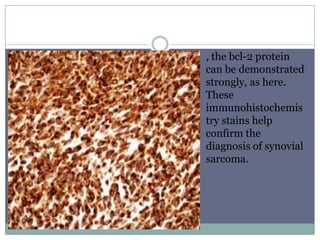
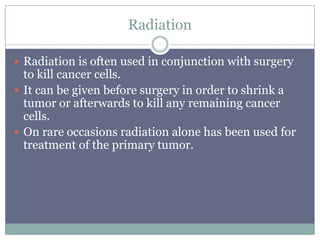
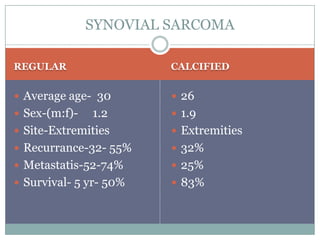


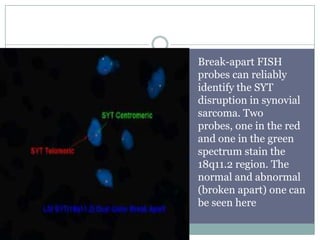
This document discusses synovial sarcoma, a rare soft tissue tumor. Key points: - It typically occurs near joints in young adults and has a slight male predominance. - Though called "synovial sarcoma", the cells it develops from are unknown and it has no relationship to normal synovium tissue. - Diagnosis involves identifying the characteristic translocation between chromosomes 18 and X via cytogenetic testing. - Treatment typically involves surgery to remove the tumor along with radiation and chemotherapy, but prognosis depends on factors like size, margins, and metastasis.



































































































