Downloaded 53 times

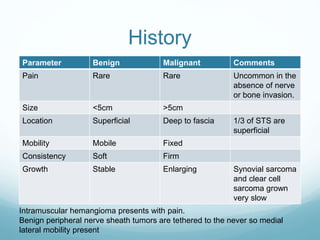
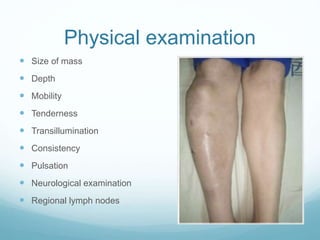
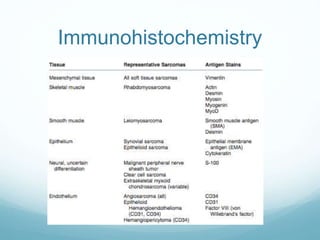
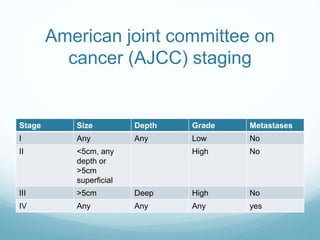
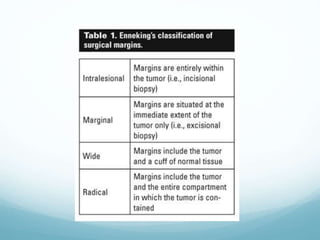


Soft tissue sarcoma is a rare group of tumors with a variety of subtypes, accounting for less than 1% of all cancers, predominantly affecting younger males and mainly located in the extremities. The document outlines the classification, diagnostic methods, treatment approaches, and prognostic factors related to soft tissue sarcomas, emphasizing the importance of accurate biopsy and surgical resection with the potential for adjuvant therapies. Additionally, it highlights that any mass over 5 cm should be treated as a soft tissue sarcoma unless otherwise proven.













































































