Downloaded 231 times
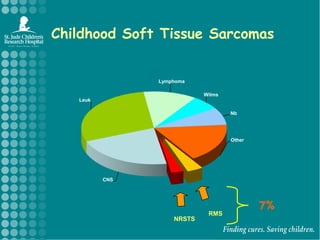
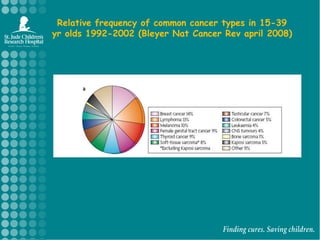
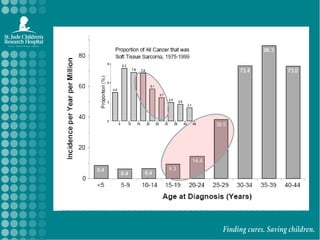
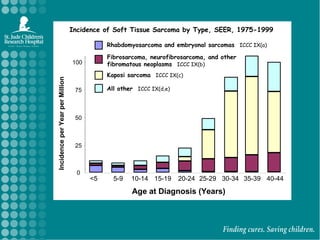
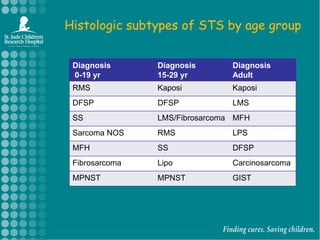
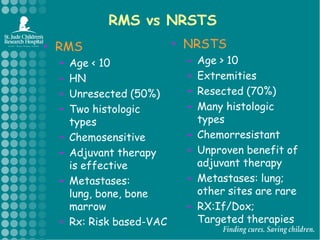
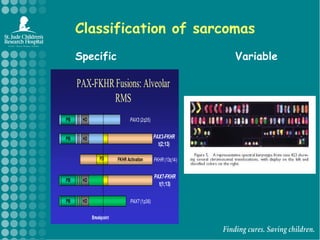
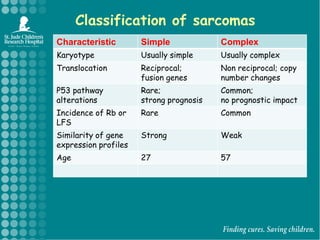
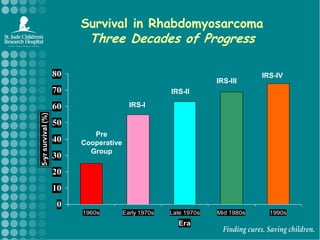
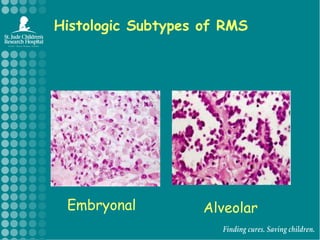
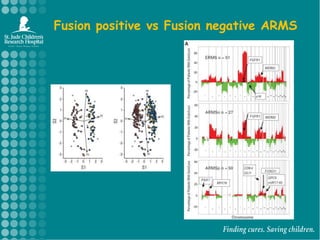
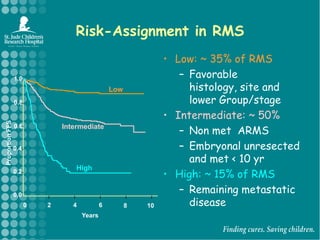
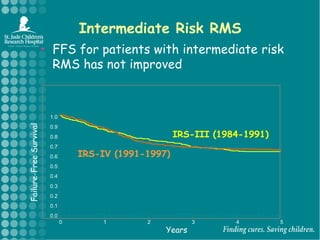
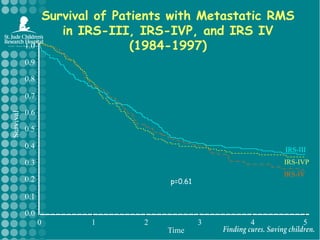
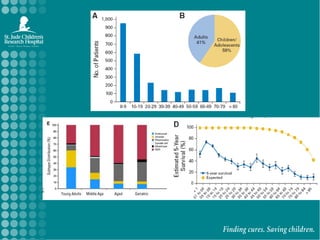
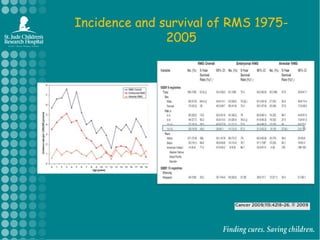
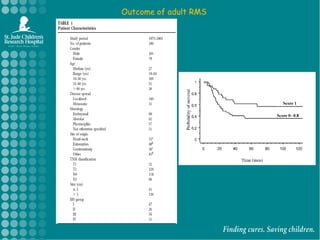
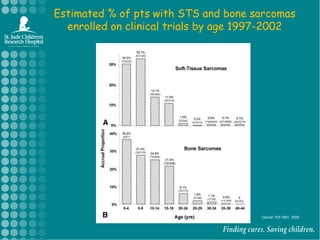
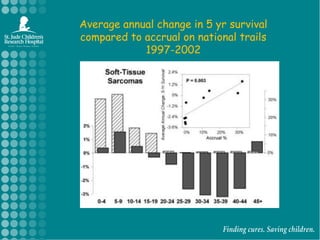
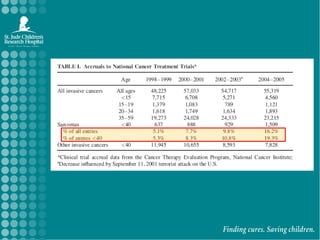
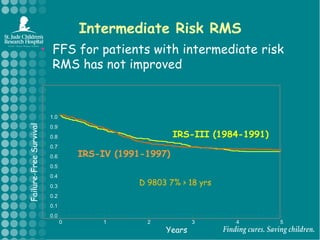
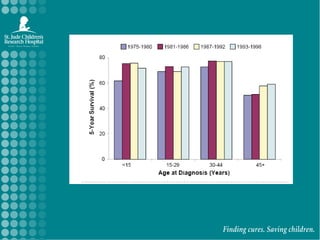
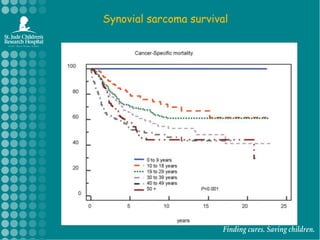
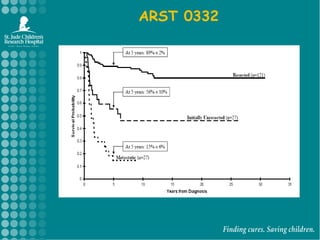
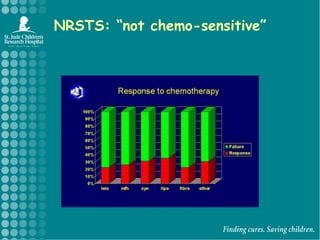
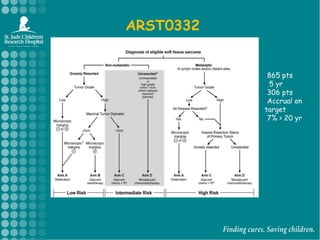
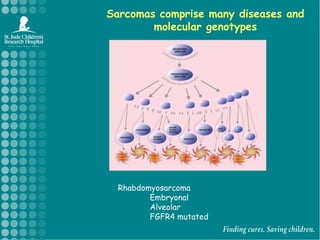
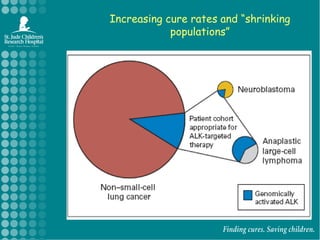
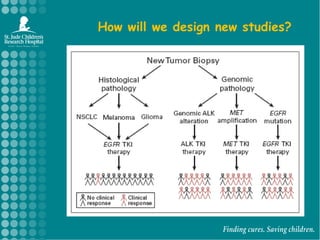
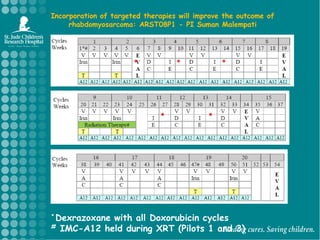

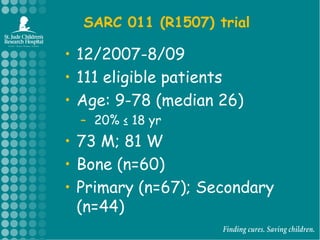
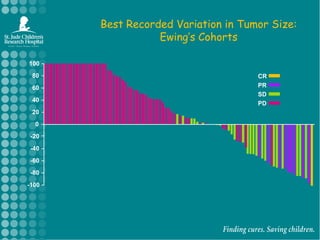

The document discusses soft tissue sarcomas (STS) in adolescents and young adults, highlighting the relative frequencies, histologic subtypes, treatment approaches, and survival outcomes for specific types, particularly rhabdomyosarcoma (RMS). It emphasizes the challenges in clinical trial enrollment and the need for collaboration between adult and pediatric oncology to improve treatment efficacy and outcomes. The piece addresses the importance of targeted therapies and ongoing research efforts to enhance understanding and treatment of these cancers.































































































