Downloaded 41 times
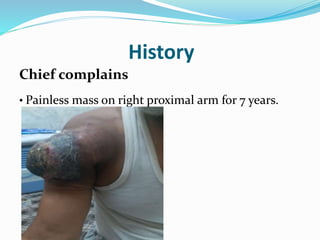
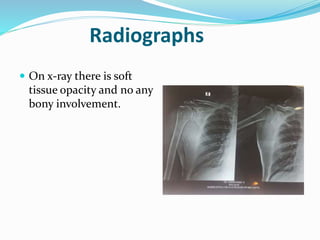
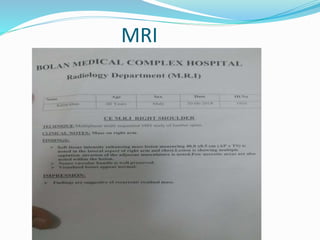
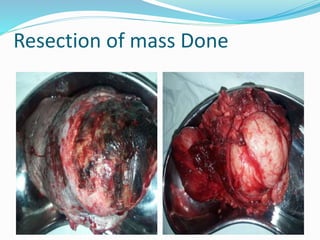



A 60-year-old male laborer presented with a recurrent soft tissue sarcoma on his right proximal arm that had been growing over 7 years. He had previously undergone 3 surgeries and chemotherapy/radiation for the mass. Examination found a large, necrotic mass with normal neurovascular function. Biopsy confirmed a low-grade soft tissue sarcoma. The management plan was a wide excision with reconstruction to remove the recurrent tumor.













































































