Download to read offline

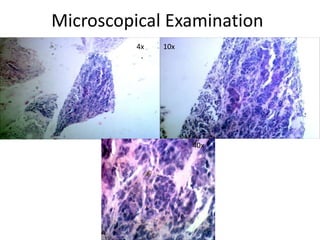
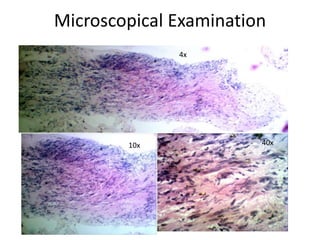


The document discusses the case of a 70-year-old male with a soft tissue tumor in his right leg. Biopsy results showed a poorly differentiated spindle cell sarcoma. Special stains and morphology were more consistent with synovial sarcoma. All surgical margins were free of tumor and lymph nodes were negative. Synovial sarcoma is an aggressive tumor most commonly found in young adults near joints. It can be diagnosed through histology showing a biphasic pattern and presence of specific gene fusions. Prognosis is poorer with larger tumor size, high grade features and metastasis.



































































